

Hypophosphatemia in cancer patients
- PMID: 34754427
- PMCID: PMC8572986
- DOI: 10.1093/ckj/sfab078
Hypophosphatemia in cancer patients
Abstract
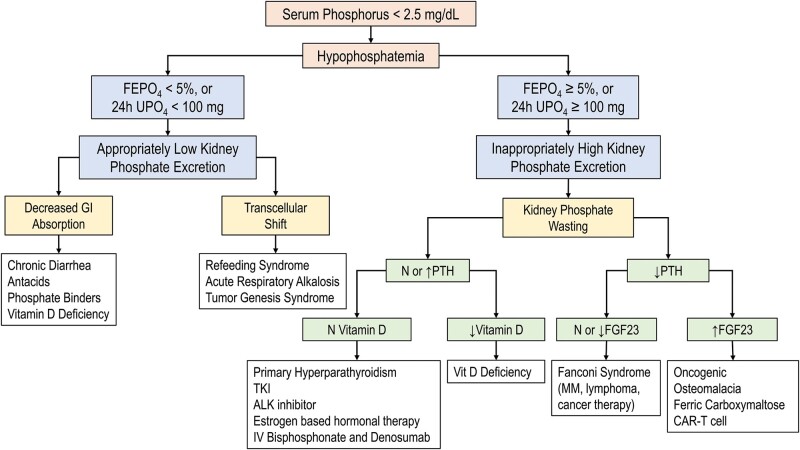
Dysregulation of phosphorus homeostasis resulting in hypophosphatemia is common in cancer patients and can result in serious complications and impact outcomes. Several factors, including critical illness, nutritional status, cancer type and therapy, influence the development of hypophosphatemia. Hypophosphatemia can develop as a result of phosphaturic mesenchymal tumors or as a paraneoplastic phenomenon. The clinical presentation for hypophosphatemia varies depending on the duration and severity of the hypophosphatemia and affects several organ systems. Among other serious effects, hypophosphatemia can impair tissue oxygenation and can cause hemolysis, leukocyte and platelet dysfunction, encephalopathy, seizures, arrhythmias, cardiomyopathy, rhabdomyolysis and coma. Multiple studies have demonstrated that hypophosphatemia is an adverse prognostic marker in inpatients with increased in-hospital stay, mortality and postoperative complications. The phosphate level is homeostatically regulated and maintained in a narrow range by three main hormones: parathyroid hormone, fibroblast growth factor 23 and 1,25-dihydroxyvitaminD3. Together, these hormones regulate how the intestine, kidneys and bones traffic phosphorus. Several hematological malignancies and cancer therapies are associated with proximal tubular dysfunction (Fanconi syndrome), resulting in phosphaturia. Caution should be taken with parenteral administration of phosphate salts, because secondary complications can develop, principally due to hypocalcemia. The general approach to hypophosphatemia should target the underlying cause. Early recognition and prevention are essential and the approach to hypophosphatemia in the cancer patient, because of the nuances and complexity, should be multidisciplinary.
Keywords: Fanconi syndrome; electrolytes; hypophosphatemia; onconephrology; phosphate; phosphaturia; phosphorus.
© The Author(s) 2021. Published by Oxford University Press on behalf of ERA-EDTA.
Figures


References
-
- Yoshida T, Taguchi D, Fukuda Ket al. . Incidence of hypophosphatemia in advanced cancer patients: a recent report from a single institution. Int J Clin Oncol 2017; 22: 244–249 - PubMed
-
- Halevy J, Bulvik S.. Severe hypophosphatemia in hospitalized patients. Arch Intern Med 1988; 148: 153–155 - PubMed
-
- Hoffmann M, Zemlin AE, Meyer WPet al. . Hypophosphataemia at a large academic hospital in South Africa. J Clin Pathol 2008; 61: 1104–1107 - PubMed
-
- Shor R, Halabe A, Rishver Set al. . Severe hypophosphatemia in sepsis as a mortality predictor. Ann Clin Lab Sci 2006; 36: 67–72 - PubMed
LinkOut - more resources
Full Text Sources
