

doi: 10.1016/j.eats.2021.07.014.
eCollection 2021 Oct.
Modified Arthroscopic Latarjet Procedure: Button Fixation Without Splitting of the Subscapularis
Affiliations
- PMID: 34754746
- PMCID: PMC8556670
- DOI: 10.1016/j.eats.2021.07.014
Item in Clipboard
Modified Arthroscopic Latarjet Procedure: Button Fixation Without Splitting of the Subscapularis
Arthrosc Tech.
.
Abstract
The Latarjet procedure is used for the treatment of anterior glenohumeral instability in the presence of bone loss. One decade after a fully arthroscopic Latarjet procedure was described, this technique has been modified to reduce the risk of complications and improve the fixation method. We aimed to simplify the components of this surgical procedure.
© 2021 by the Arthroscopy Association of North America. Published by Elsevier.
Figures
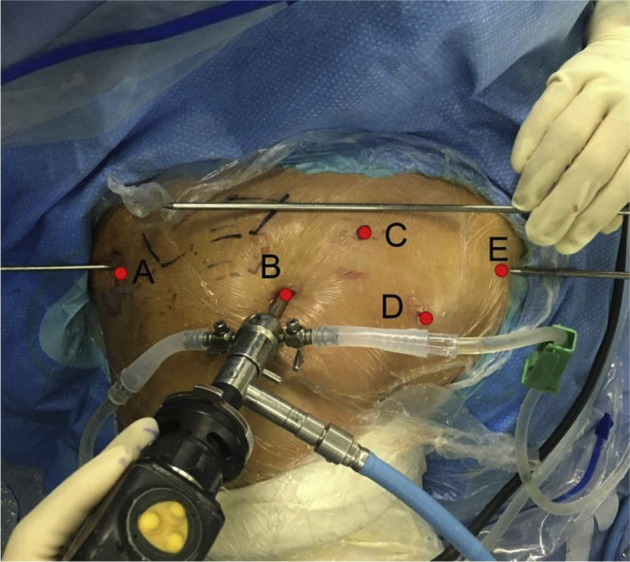
Arthroscopic portals of a right shoulder in the “beach chair” position. The posterior (A) portal was 2-cm inferior and 1-cm medial to the posterolateral angle of the acromion. The superolateral portal (B) was located 1-cm anterior and 1-cm lateral to the anterolateral corner of the acromion. The supracoracoid portal (C) was located above the base of the coracoid bone. The infracoracoid portal (D) was established under observation through portal A. Portal D was located in the axillary fold, 5-cm distal to the coracoid tip, and in the middle of conjoined tendon. The medial inferior portal (E) was created along the parallel line of portal A, When making portal E, we entered an switching stick from the posterior approach as a guide, and the switching stick points to 4’o clock direction of the glenoid rim. An switching stick was used outside the joint parallel to the direction of the switching stick inside the joint. Under the guidance of the two switching sticks, the B portal was used for observation, the puncture needle was entered in the antero medial direction. In the joint, it needs to see that the puncture needle is parallel to the switching stick inside, and the height is at the 4 o’clock level of the glenoid rim. Then make a skin incision.
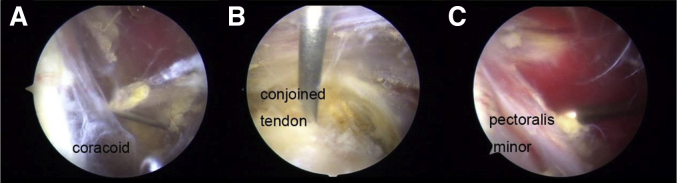
Arthroscopic view of portals C, D, and E. (A) The arthroscopic view of portal D was in the middle of the conjoined tendon. (B) The supracoracoid portal C was created under the view of portal D under the guidance of a puncture needle. (C) The medial inferior portal E was created to separate the pectoralis minor.
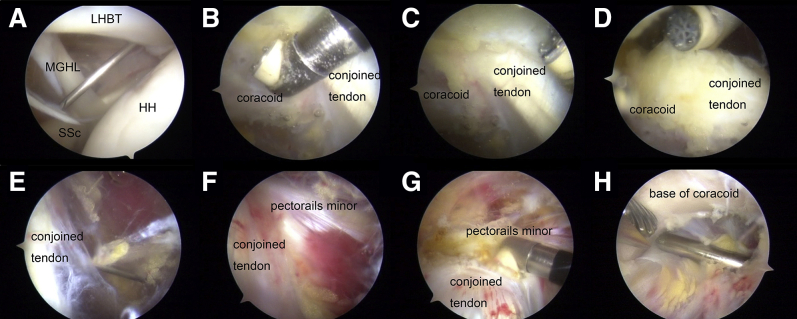
Separation of the coracoid. A. Arthroscopic view from portal A in a right shoulder in the beach chair position showing the creation of portal B. (B) A radiofrequency were used to separate the conjoined tendon and the tip and the lower surface of the coracoid under the arthroscopic view from portal A. (C) The upper surface of the coracoid were separated by cut off coracoacromial ligament. D. Separation of the upper surface of the coracoid. E. Portal D were created under the arthroscopic view from portal B. F. Identification of the conjoined tendon and separation of pectoralis minor under arthroscopic view from portal B. G. The conjoined tendon and pectoralis minor were separated by a radiofrequency from portal D and view from portal B. H. Preparation of the base of the coracoid for matching the glenoid using a burr from portal A under the arthroscopic view of portal B. LHBT: long head of bicep tendon; HH: humeral head; MGHL: middle glenohumeral ligament. SSc: subscapularis.

Schedule and the arthroscopic view of coracoid drilling. A. The length of the coracoid graft was <25 mm. Two holes (2.7 mm in diameter) were drilled and were 10-mm apart. B. A thin cannula from portal C was used to guide the drilling of two holes in the coracoid bone. A needle with PDS line inserted was pass through the hole (C) and the PDS line was pull out from the base of the coracoid (D).

Osteotomy of the coracoid bone. Schedule of coracoid osteotomy (A). Arthroscopic view from the B portal in a right shoulder in the beach chair position. PDS lines were passed through the two holes, and the osteotomy was undertaken using an osteotome (A and B). Image (C) shows the osteotomized coracoid bone.

Glenoid preparation. Arthroscopic view from the B portal in a right shoulder in the beach chair position. A. The capsule was attached to the glenoid before separation. B. The capsule was separated by a shovel. C. The glenoid were exposed to 6 o’clock at least. D. In order to match the transferred coracoid and to create better healing processs, the anterior face of the glenoid was refreshed by a burr after separation. E. The glenoid was exposed enough and finished separation. F. The subscapularis was press down by switching stick to expose the anterior face of glenoid.

Drilling of glenoid tunnels. Schedule of drilling of glenoid tunnels (A). Arthroscopic view from portal D. The subscapularis muscle is pressed downwards by an switching stick. The guide was entry from portal E and a tunnel was drilled in the 3:30 o’clock position (B). SSc, subscapularis.

Button modification. There was a long button, a round button, and a suture in the modified button (A). The long buttons were passed through the coracoid bone and from the anterior to posterior directions of the glenoid bone (B) and tightened (C).

The position of the transferred coracoid. Schedule of the coracoid and the subscapularis after fixation (A and B). Arthroscopic view of the transferred coracoid, a round button was ready to be tightened (C). Arthroscopic view from the A portal in a right shoulder in the beach chair position shows the final positioning of the transferred coracoid. Graft is flush to the glenoid margin. (D).

Radiograph and 3D-CT showing the postoperative position of the coracoid. A. Right shoulder. Postoperative anteroposterior view shows the coracoid fixed with 2 buttons. B and C. 3D-CT image shows the correct position of the graft. Black arrows: long buttons; white arrows: round buttons; red arrows: the transferred coracoid.
References
-
- Balg F., Boileau P. The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. J Bone Joint Surg Br. 2007;89:1470–1477. - PubMed
-
- Wong S.E., Friedman L.G.M., Garrigues G.E. Arthroscopic Latarjet: Indications, Techniques, and Results. Arthroscopy. 2020;36:2044–2046. - PubMed
-
- Vezeridis P.S., Ishmael C.R., Jones K.J., Petrigliano F.A. Glenohumeral Dislocation Arthropathy: Etiology, Diagnosis, and Management. J Am Acad Orthop Surg. 2019;27:227–235. - PubMed
-
- Lafosse L., Lejeune E., Bouchard A., Kakuda C., Gobezie R., Kochhar T. The arthroscopic Latarjet procedure for the treatment of anterior shoulder instability. Arthroscopy. 2007;23 1242 e1241-1245. - PubMed
LinkOut - more resources
Full Text Sources
