

Association Between Thrombogenicity Indices and Coronary Microvascular Dysfunction in Patients With Acute Myocardial Infarction
- PMID: 34754989
- PMCID: PMC8559320
- DOI: 10.1016/j.jacbts.2021.08.007
Association Between Thrombogenicity Indices and Coronary Microvascular Dysfunction in Patients With Acute Myocardial Infarction
Abstract
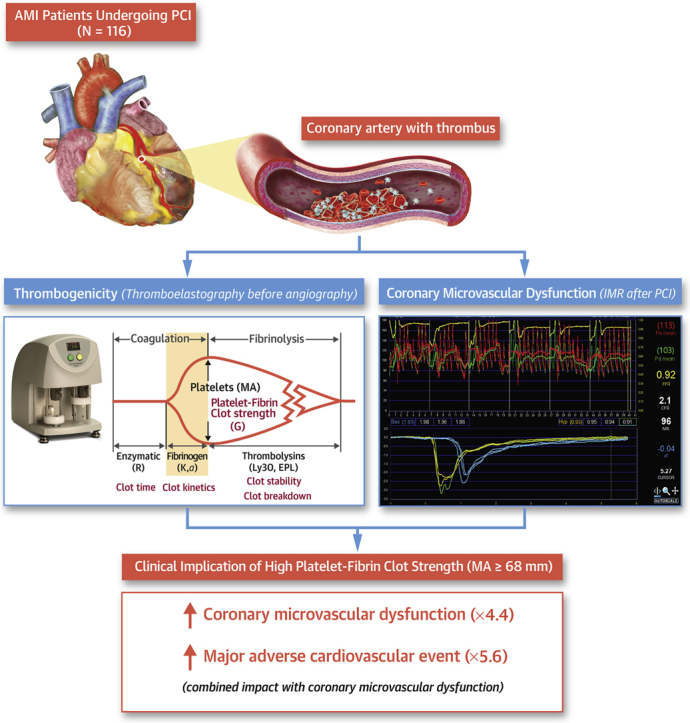
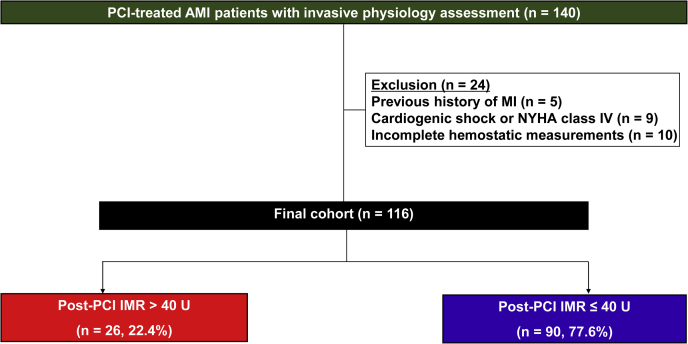
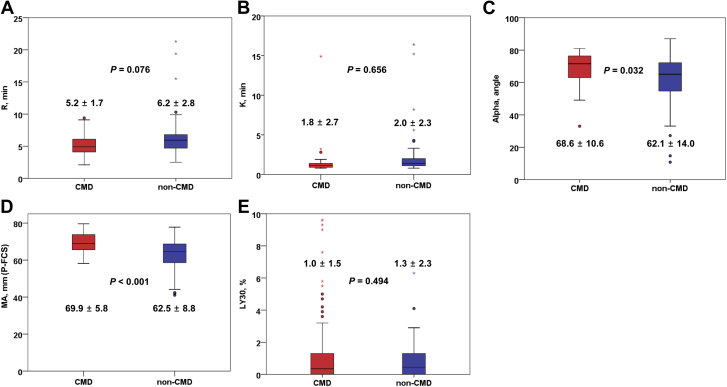
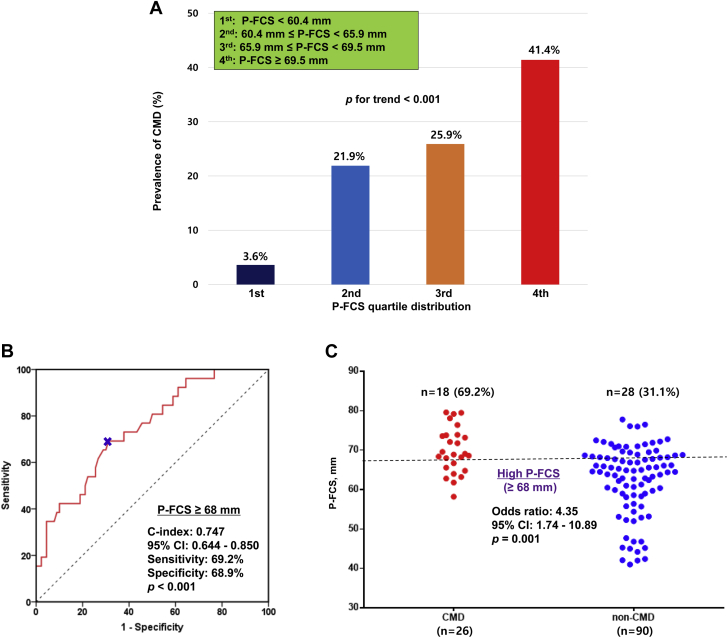
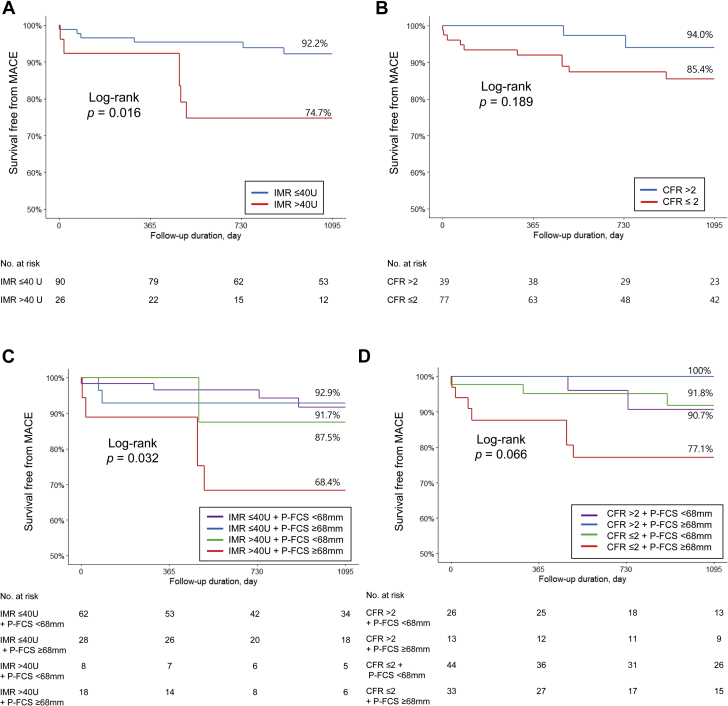
The association between thrombogenicity and coronary microvascular dysfunction (CMD) has been poorly explored in patients with acute myocardial infarction (AMI). In our real-world clinical practice (N = 116), thrombogenicity was evaluated with thromboelastography and conventional hemostatic measures, and CMD was defined as index of microcirculatory resistance of >40 U using the invasive physiologic test. High platelet-fibrin clot strength (P-FCS) (≥68 mm) significantly increased the risk of postprocedural CMD (odds ratio: 4.35; 95% CI: 1.74-10.89). Patients with both CMD and high P-FCS had a higher rate of ischemic events compared to non-CMD subjects with low P-FCS (odds ratio: 5.58; 95% CI: 1.31-23.68). This study showed a close association between heightened thrombogenicity and CMD and their prognostic implications after reperfusion in acute myocardial infarction patients.
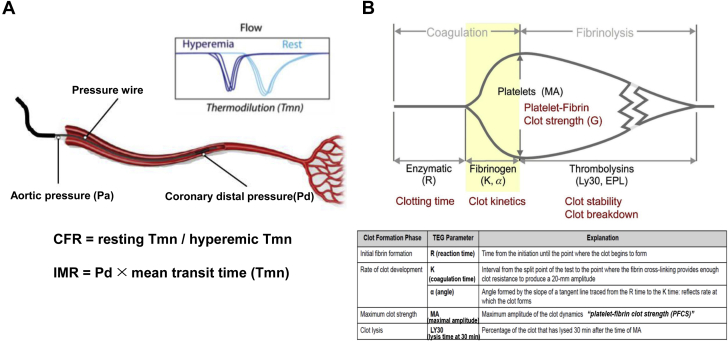
Keywords: AMI, acute myocardial infarction; CFR, coronary flow reserve; CMD, coronary microvascular dysfunction; IMR, index of microcirculatory resistance; LASSO, least absolute shrinkage and selection operator; MA, maximum amplitude; MACE, major adverse cardiovascular events; OR, odds ratio; P-FCS, platelet-fibrin clot strength; PCI, percutaneous coronary intervention; PRU, P2Y12 reaction units; R, reaction time; TEG, thromboelastography; TIMI, Thrombolysis in Myocardial Infarction; Tmn, mean transit time; acute myocardial infarction; cardiovascular event; clot strength; coronary microvascular dysfunction; thrombogenicity.
© 2021 The Authors.
Conflict of interest statement
This study was supported by the Basic Science Research Program through the National Research Foundation (NRF) of Korea funded by the Ministry of Science, ICT, and Future Planning (NRF-2015R1A5A2008833). The content is solely the responsibility of the authors and does not necessarily represent the official views of any funding agencies. Dr Gurbel has received grants and personal fees from Bayer HealthCare, Otitopic, Amgen, and Janssen, US WorldMeds; grants from Instrumentation Laboratory, Hikari Dx, Haemonetics, Medicure, and Idorsia Pharmaceuticals; and personal fees from UpToDate and has patents “Detection of Restenosis Risk in Patients Issued” and “Assessment of Cardiac Health and Thrombotic Risk in a Patient.” Dr Jeong has received honoraria for lectures from AstraZeneca, Daiichi Sankyo, Sanofi-Aventis, Han-mi Pharmaceuticals, and Yuhan Pharmaceuticals and research grants or support from Yuhan Pharmaceuticals and U and I Corporation. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Pfeffer M.A., Braunwald E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation. 1990;81:1161–1172. - PubMed
-
- Fearon W.F., Balsam L.B., Farouque H.M. Novel index for invasively assessing the coronary microcirculation. Circulation. 2003;107:3129–3132. - PubMed
-
- de Waha S., Patel M.R., Granger C.B. Relationship between microvascular obstruction and adverse events following primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: an individual patient data pooled analysis from seven randomized trials. Eur Heart J. 2017;38:3502–3510. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
