

Device-Based Solutions to Improve Cardiac Physiology and Hemodynamics in Heart Failure With Preserved Ejection Fraction
- PMID: 34754993
- PMCID: PMC8559325
- DOI: 10.1016/j.jacbts.2021.06.002
Device-Based Solutions to Improve Cardiac Physiology and Hemodynamics in Heart Failure With Preserved Ejection Fraction
Abstract
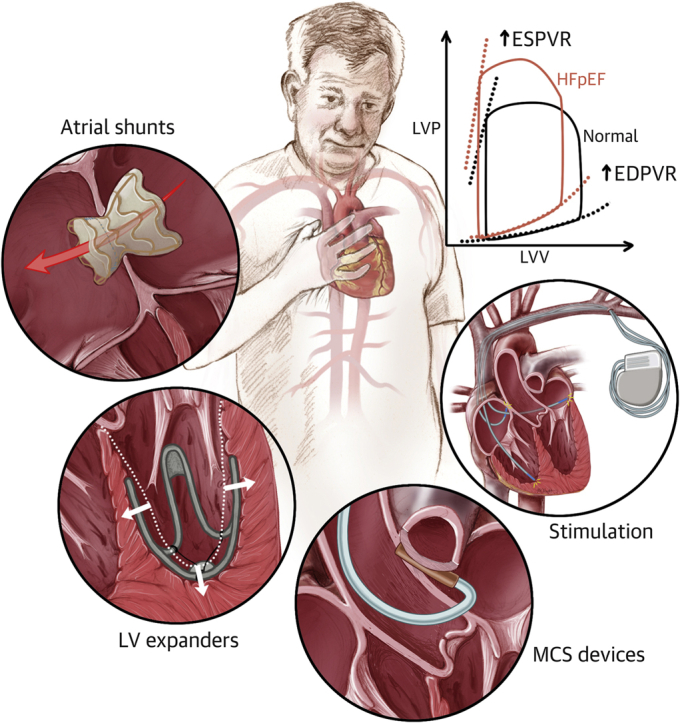
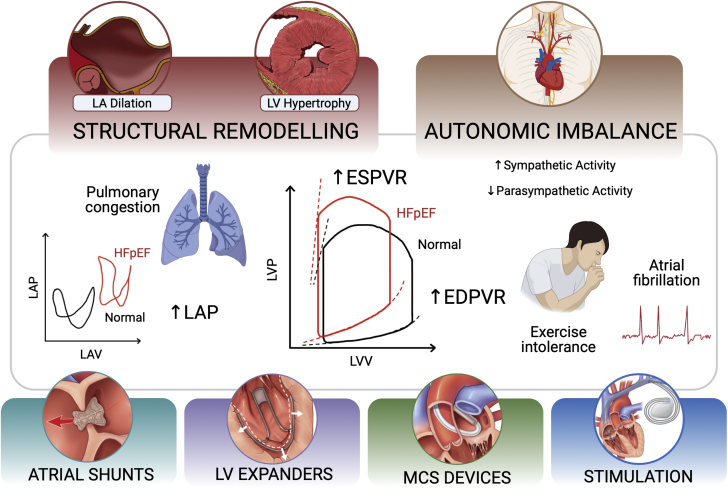
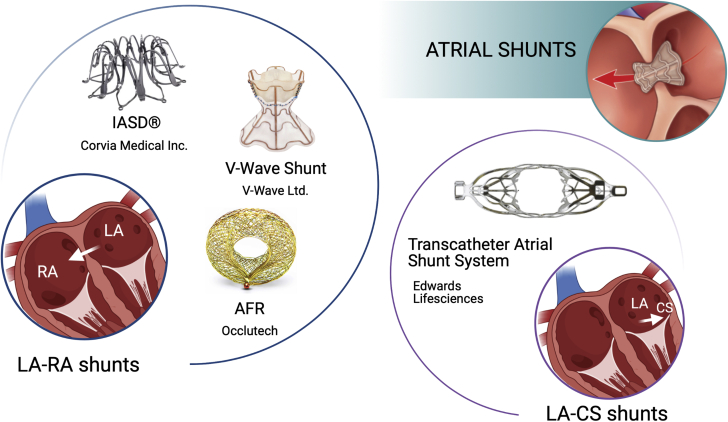
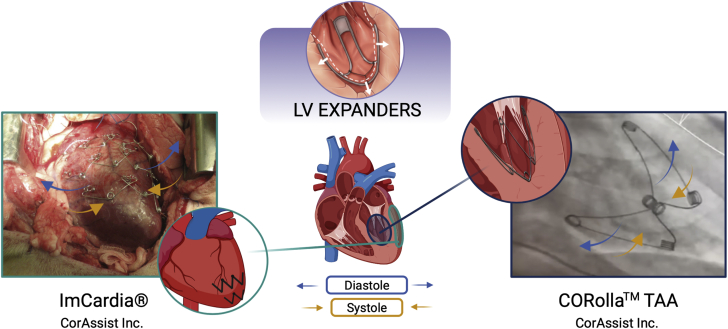
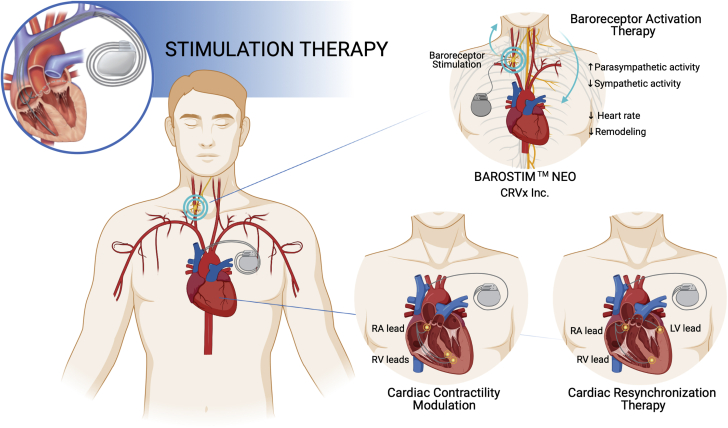
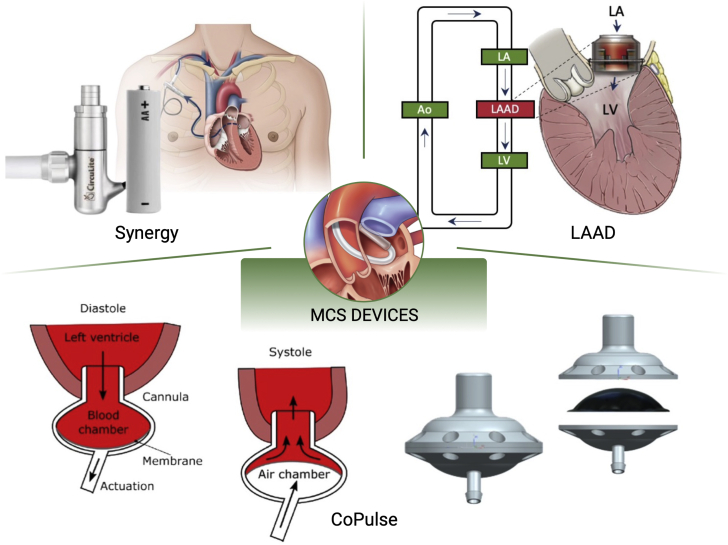
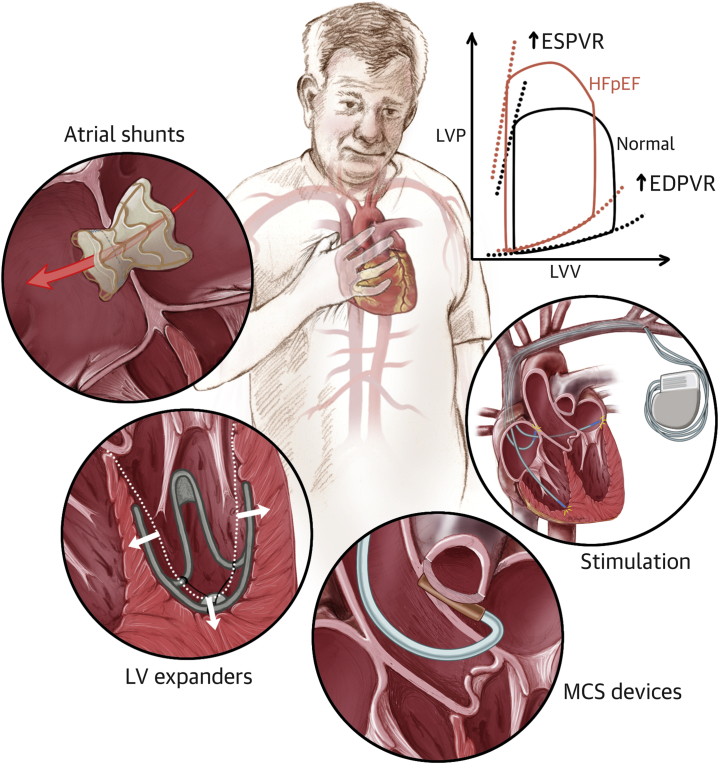
Characterized by a rapidly increasing prevalence, elevated mortality and rehospitalization rates, and inadequacy of pharmaceutical therapies, heart failure with preserved ejection fraction (HFpEF) has motivated the widespread development of device-based solutions. HFpEF is a multifactorial disease of various etiologies and phenotypes, distinguished by diminished ventricular compliance, diastolic dysfunction, and symptoms of heart failure despite a normal ejection performance; these symptoms include pulmonary hypertension, limited cardiac reserve, autonomic imbalance, and exercise intolerance. Several types of atrial shunts, left ventricular expanders, stimulation-based therapies, and mechanical circulatory support devices are currently under development aiming to target one or more of these symptoms by addressing the associated mechanical or hemodynamic hallmarks. Although the majority of these solutions have shown promising results in clinical or preclinical studies, no device-based therapy has yet been approved for the treatment of patients with HFpEF. The purpose of this review is to discuss the rationale behind each of these devices and the findings from the initial testing phases, as well as the limitations and challenges associated with their clinical translation.
Keywords: BAT, baroreceptor activation therapy; CCM, cardiac contractility modulation; CRT, cardiac resynchronization therapy; HF, heart failure; HFmEF, heart failure with mid-range ejection fraction; HFpEF; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; IASD, Interatrial Shunt Device; LAAD, left atrial assist device; LAP, left atrial pressure; LV, left ventricular; LVEF, left ventricular ejection fraction; MCS, mechanical circulatory support; NYHA, New York Heart Association; PCWP, pulmonary capillary wedge pressure; QoL, quality of life; TAA, transapical approach; atrial shunt devices; electrostimulation; heart failure devices; heart failure with preserved ejection fraction; left ventricular expanders; mechanical circulatory support; neuromodulation.
© 2021 The Authors.
Conflict of interest statement
Dr Hameed is leading a project to develop a novel device for HFpEF. The project is funded by the Enterprise Ireland through their Commercialization Fund (CF-2019-1136-P). This project is co-funded by the European Regional Development Fund under Ireland’s European Structural and Investment Funds Programme 2014-2020. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Yusuf S., Rangarajan S., Teo K. Cardiovascular risk and events in 17 low-, middle-, and high-income countries. N Engl J Med. 2014;371(9):818–827. - PubMed
-
- Yancy C.W., Jessup M., Bozkurt B. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2013;62(16):e147–e239. - PubMed
-
- Yancy C.W., Jessup M., Bozkurt B. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinic. J Am Coll Cardiol. 2016;68(13):1476–1488. - PubMed
-
- Borlaug B.A. Evaluation and management of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2020;17:559–573. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
