A methodology for identifying high-need, high-cost patient personas for international comparisons
- PMID: 34755334
- PMCID: PMC8579201
- DOI: 10.1111/1475-6773.13890
A methodology for identifying high-need, high-cost patient personas for international comparisons
Abstract
Objective: To establish a methodological approach to compare two high-need, high-cost (HNHC) patient personas internationally.
Data sources: Linked individual-level administrative data from the inpatient and outpatient sectors compiled by the International Collaborative on Costs, Outcomes, and Needs in Care (ICCONIC) across 11 countries: Australia, Canada, England, France, Germany, the Netherlands, New Zealand, Spain, Sweden, Switzerland, and the United States.
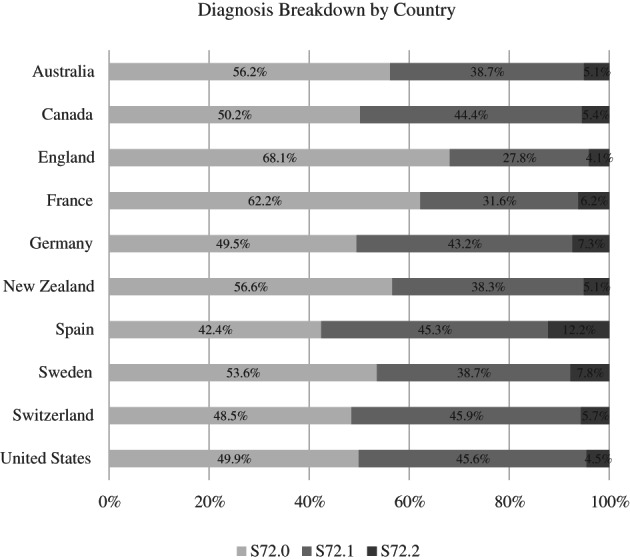
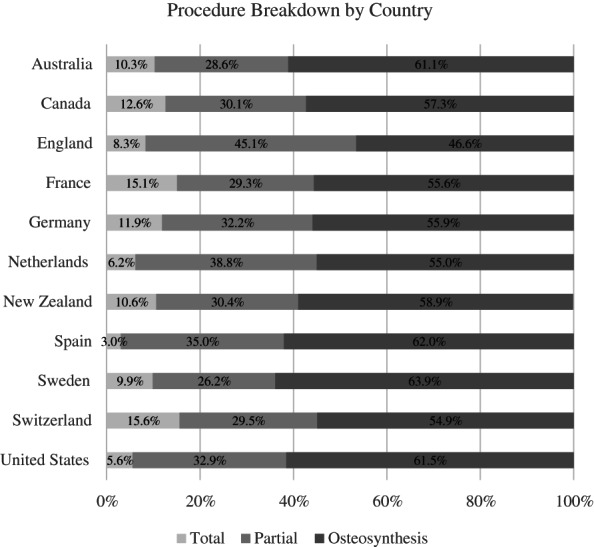
Study design: We outline a methodological approach to identify HNHC patient types for international comparisons that reflect complex, priority populations defined by the National Academy of Medicine. We define two patient profiles using accessible patient-level datasets linked across different domains of care-hospital care, primary care, outpatient specialty care, post-acute rehabilitative care, long-term care, home-health care, and outpatient drugs. The personas include a frail older adult with a hip fracture with subsequent hip replacement and an older person with complex multimorbidity, including heart failure and diabetes. We demonstrate their comparability by examining the characteristics and clinical diagnoses captured across countries.
Data collection/extraction methods: Data collected by ICCONIC partners.
Principal findings: Across 11 countries, the identification of HNHC patient personas was feasible to examine variations in healthcare utilization, spending, and patient outcomes. The ability of countries to examine linked, individual-level data varied, with the Netherlands, Canada, and Germany able to comprehensively examine care across all seven domains, whereas other countries such as England, Switzerland, and New Zealand were more limited. All countries were able to identify a hip fracture persona and a heart failure persona. Patient characteristics were reassuringly similar across countries.
Conclusion: Although there are cross-country differences in the availability and structure of data sources, countries had the ability to effectively identify comparable HNHC personas for international study. This work serves as the methodological paper for six accompanying papers examining differences in spending, utilization, and outcomes for these personas across countries.
Keywords: international comparison; vignettes.
© 2021 The Authors. Health Services Research published by Wiley Periodicals LLC on behalf of Health Research and Educational Trust.
Figures