

Risk factors associated with pulmonary hypertension in obesity hypoventilation syndrome
- PMID: 34755598
- PMCID: PMC8974388
- DOI: 10.5664/jcsm.9760
Risk factors associated with pulmonary hypertension in obesity hypoventilation syndrome
Abstract
Study objectives: Pulmonary hypertension (PH) is prevalent in obesity hypoventilation syndrome (OHS). However, there is a paucity of data assessing pathogenic factors associated with PH. Our objective is to assess risk factors that may be involved in the pathogenesis of PH in untreated OHS.
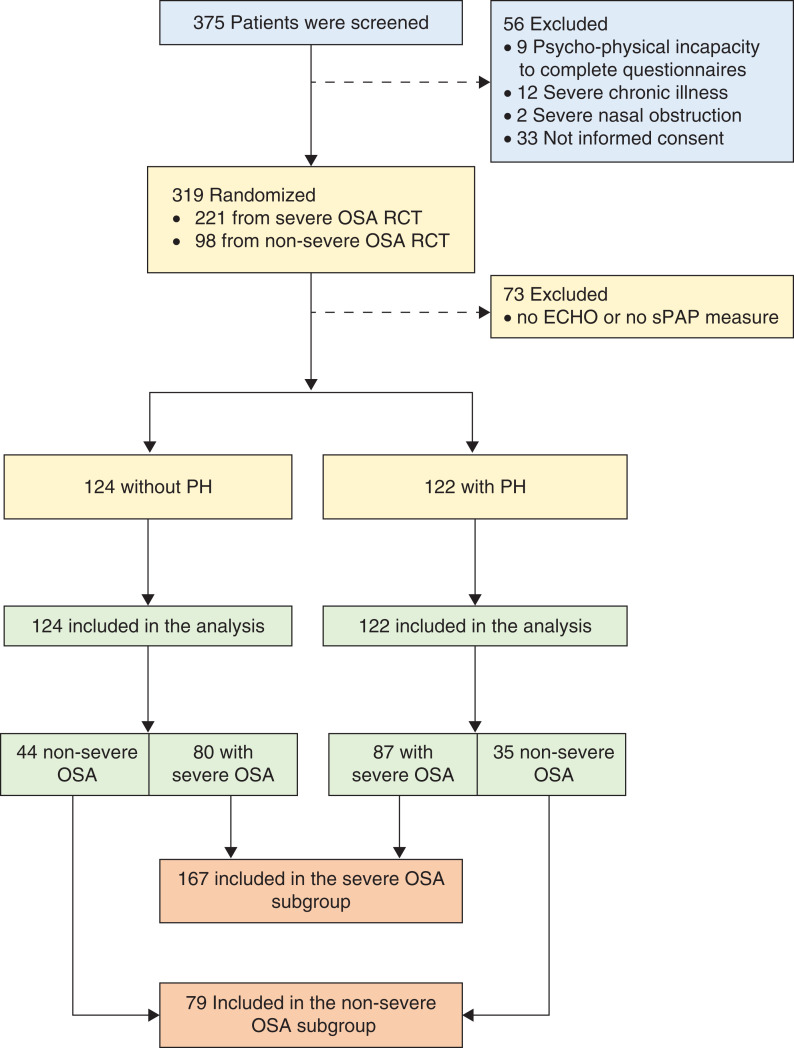
Methods: In a post hoc analysis of the Pickwick trial, we performed a bivariate analysis of baseline characteristics between patients with and without PH. Variables with a P value ≤ .10 were defined as potential risk factors and were grouped by theoretical pathogenic mechanisms in several adjusted models. Similar analysis was carried out for the 2 OHS phenotypes, with and without severe concomitant obstructive sleep apnea.
Results: Of 246 patients with OHS, 122 (50%) had echocardiographic evidence of PH defined as systolic pulmonary artery pressure ≥ 40 mm Hg. Lower levels of awake PaO2 and higher body mass index were independent risk factors in the multivariate model, with a negative and positive adjusted linear association, respectively (adjusted odds ratio 0.96; 95% confidence interval 0.93 to 0.98; P = .003 for PaO2, and 1.07; 95% confidence interval 1.03 to 1.12; P = .001 for body mass index). In separate analyses, body mass index and PaO2 were independent risk factors in the severe obstructive sleep apnea phenotype, whereas body mass index and peak in-flow velocity in early/late diastole ratio were independent risk factors in the nonsevere obstructive sleep apnea phenotype.
Conclusions: This study identifies obesity per se as a major independent risk factor for PH, regardless of OHS phenotype. Therapeutic interventions targeting weight loss may play a critical role in improving PH in this patient population.
Clinical trial registration: Registry: Clinicaltrial.gov; Name: Alternative of Treatment in Obesity Hypoventilation Syndrome; URL: https://clinicaltrials.gov/ct2/show/NCT01405976; Identifier: NCT01405976.
Citation: Masa JF, Benítez ID, Javaheri S, et al. Risk factors associated with pulmonary hypertension in obesity hypoventilation syndrome. J Clin Sleep Med. 2022;18(4):983-992.
Keywords: CPAP; hypercapnia; hypoxemia; noninvasive ventilation; sleep apnea.
© 2022 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved this manuscript. This study was funded by Instituto de Salud Carlos III (Fondo de Investigaciones Sanitarias, Ministerio de Sanidad y Consumo) PI050402, Spanish Respiratory Foundation 2005 (FEPAR), and Air Liquide Spain. The sponsors and funders of the study had no involvement or any influence in study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for publication. The corresponding author (J.F.M.) confirms that he had full access to all the data in the study and he had the final responsibility for the decision to submit for publication. The authors report no conflicts of interest.
Figures
References
-
- Kessler R , Chaouat A , Schinkewitch P , et al . The obesity-hypoventilation syndrome revisited: a prospective study of 34 consecutive cases . Chest. 2001. ; 120 ( 2 ): 369 – 376 . - PubMed
-
- Masa JF , Corral J , Alonso ML , et al. ; Spanish Sleep Network . Efficacy of different treatment alternatives for obesity hypoventilation syndrome. Pickwick Study . Am J Respir Crit Care Med. 2015. ; 192 ( 1 ): 86 – 95 . - PubMed
-
- Basoglu OK , Tasbakan MS . Comparison of clinical characteristics in patients with obesity hypoventilation syndrome and obese obstructive sleep apnea syndrome: a case-control study . Clin Respir J. 2014. ; 8 ( 2 ): 167 – 174 . - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
