

Coronary artery calcium is associated with long-term mortality from lung cancer: Results from the Coronary Artery Calcium Consortium
- PMID: 34756729
- PMCID: PMC8678296
- DOI: 10.1016/j.atherosclerosis.2021.10.007
Coronary artery calcium is associated with long-term mortality from lung cancer: Results from the Coronary Artery Calcium Consortium
Abstract
Background and aims: Coronary artery calcium (CAC) scores have been shown to be associated with CVD and cancer mortality. The use of CAC scores for overall and lung cancer mortality risk prediction for patients in the Coronary Artery Calcium Consortium was analyzed.
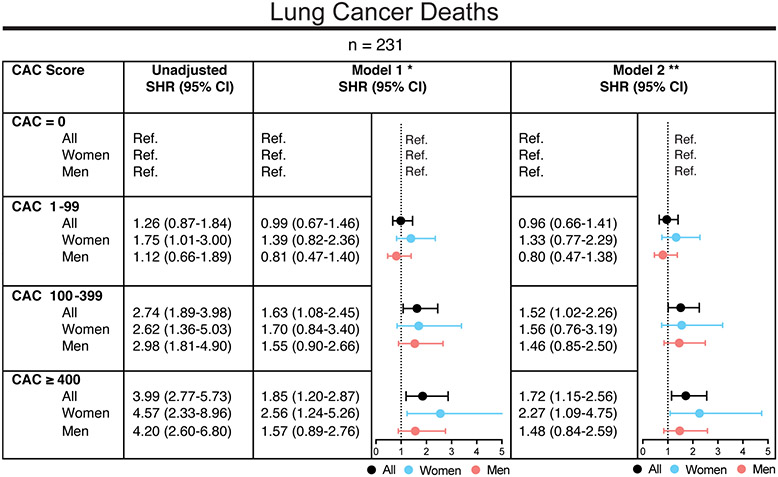
Methods: We included 55,943 patients aged 44-84 years without known heart disease from the CAC Consortium. There were 1,088 cancer deaths, among which 231 were lung cancer, identified by death certificates with a mean follow-up of 12.2 ± 3.9 years. Fine-and-Gray competing-risk regression was used for overall and lung cancer-specific mortality, accounting for the competing risk of CVD death and after adjustment for CVD risk factors. Subdistribution hazard ratios (SHR) were reported.
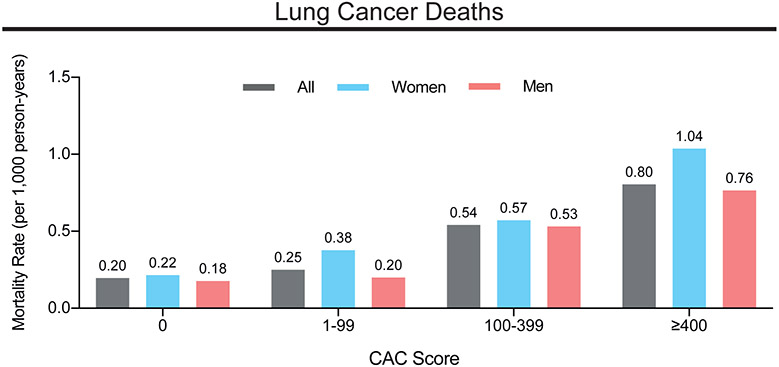
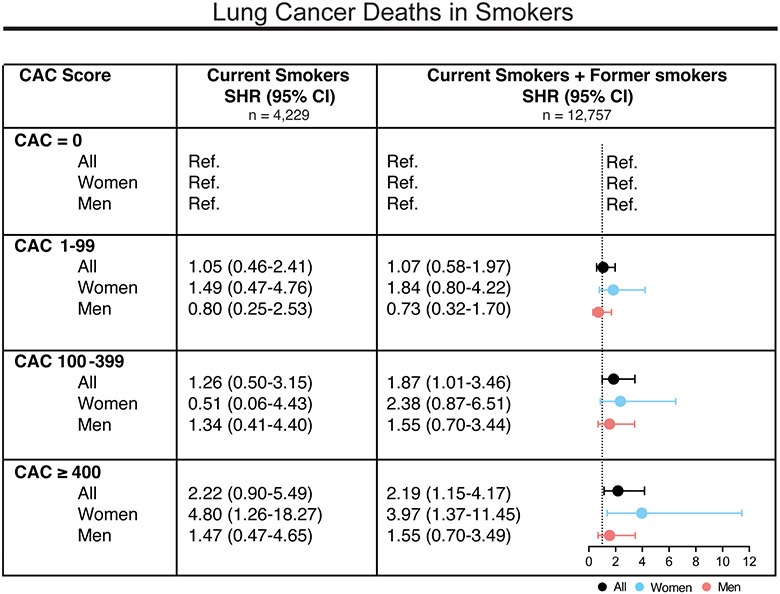
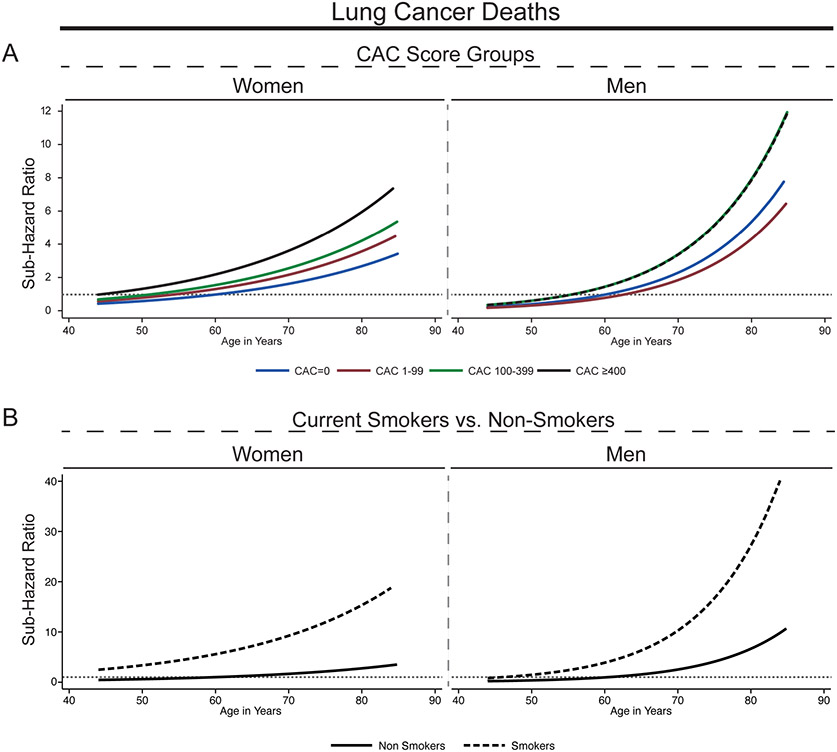
Results: The mean age of all patients was 57.1 ± 8.6 years, 34.9% were women, and 89.6% were white. Overall, CAC was strongly associated with cancer mortality. Lung cancer mortality increased with increasing CAC scores, with rates per 1000-person years of 0.2 (95% CI: 0.1-0.3) for CAC = 0 and 0.8 (95% CI: 0.6-1.0) for CAC ≥400. Compared with CAC = 0, hazards were increased for those with CAC ≥400 for lung cancer mortality [SHR: 1.7 (95% CI: 1.2-2.6)], which was driven by women [SHR: 2.3 (95% CI: 1.1-4.8)], but not significantly increased for men. Risks were higher in those with positive smoking history [SHR: 2.2 (95% CI: 1.2-4.2)], with associations driven by women [SHR: 4.0 (95% CI: 1.4-11.5)].
Conclusions: CAC scores were associated with increased risks for lung cancer mortality, with strongest associations for current and former smokers, especially in women. Used in conjunction with other clinical variables, our data pinpoint a potential synergistic use of CAC scanning beyond CVD risk assessment for identification of high-risk lung cancer screening candidates.
Keywords: Cancer; Cardiovascular disease; Coronary arterial calcium; Lung cancer; Prevention; Risk prediction.
Copyright © 2021 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Comment in
-
The mystery of coronary calcium and clinical events.Atherosclerosis. 2021 Dec;339:46-47. doi: 10.1016/j.atherosclerosis.2021.11.014. Epub 2021 Nov 17. Atherosclerosis. 2021. PMID: 34802684 No abstract available.
References
-
- Siegel RL, Miller KD and Jemal A, Cancer statistics, 2020, CA Cancer J Clin, 2020;70:7–30. - PubMed
-
- Stewart BW and Wild CP, World cancer report 2014, 2014.
-
- Islami F, Goding Sauer A, Miller KD, et al., Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States, CA Cancer J Clin, 2018;68:31–54. - PubMed
-
- Benjamin EJ, Muntner P, Alonso A, et al., Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association, Circulation, 2019;139:e56–e528. - PubMed
