

Changes in paediatric respiratory infections at a UK teaching hospital 2016-2021; impact of the SARS-CoV-2 pandemic
- PMID: 34757137
- PMCID: PMC8591975
- DOI: 10.1016/j.jinf.2021.10.022
Changes in paediatric respiratory infections at a UK teaching hospital 2016-2021; impact of the SARS-CoV-2 pandemic
Abstract
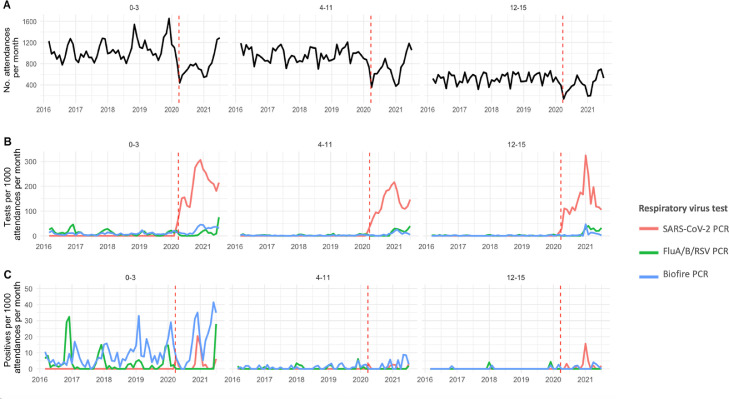
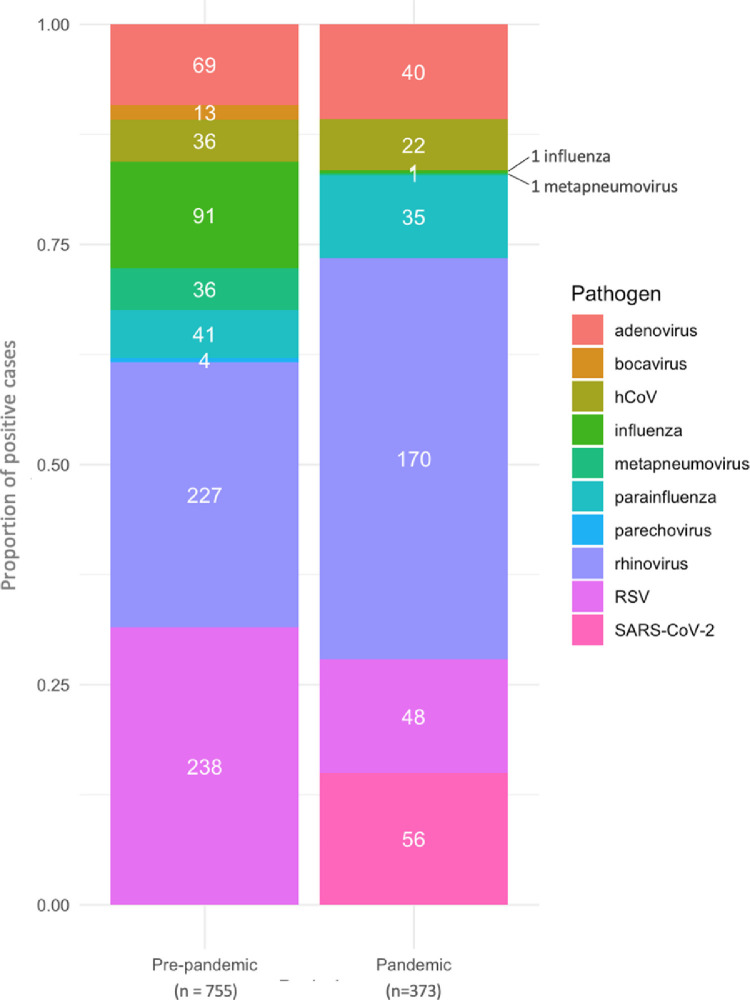
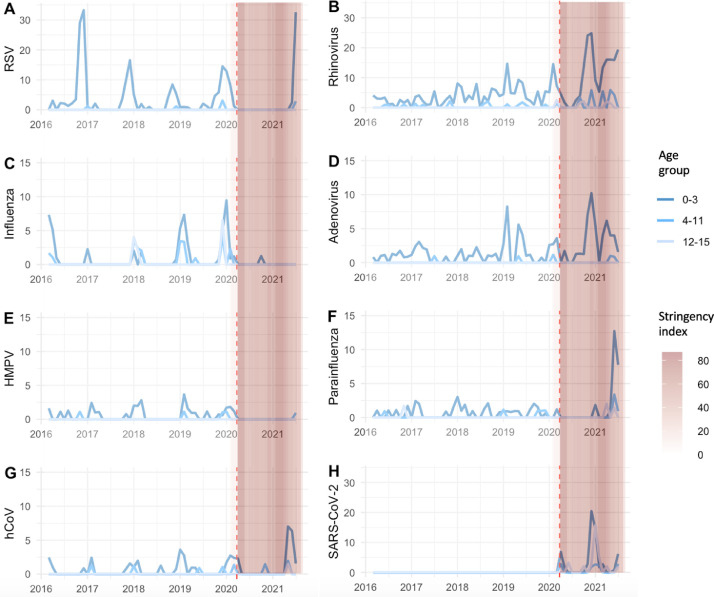
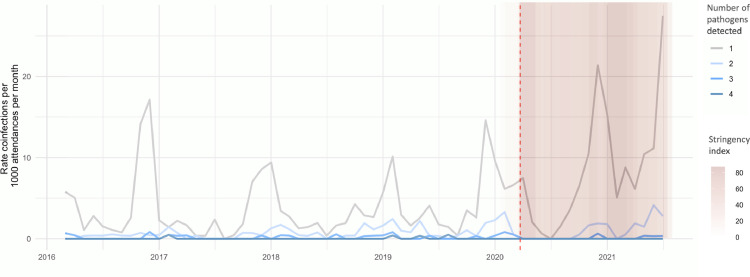
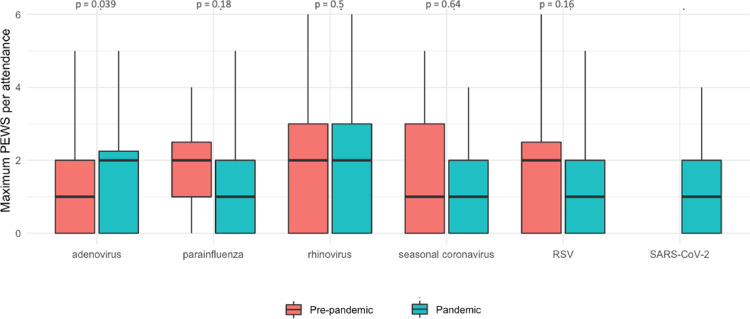
Objective To describe the impact of the SARS-CoV-2 pandemic on the incidence of paediatric viral respiratory tract infection in Oxfordshire, UK. Methods Data on paediatric Emergency Department (ED) attendances (0-15 years inclusive), respiratory virus testing, vital signs and mortality at Oxford University Hospitals were summarised using descriptive statistics. Results Between 1-March-2016 and 30-July-2021, 155,056 ED attendances occurred and 7,195 respiratory virus PCRs were performed. Detection of all pathogens was suppressed during the first national lockdown. Rhinovirus and adenovirus rates increased when schools reopened September-December 2020, then fell, before rising in March-May 2021. The usual winter RSV peak did not occur in 2020/21, with an inter-seasonal rise (32/1,000 attendances in 0-3 yr olds) in July 2021. Influenza remained suppressed throughout. A higher paediatric early warning score (PEWS) was seen for attendees with adenovirus during the pandemic compared to pre-pandemic (p = 0.04, Mann-Witney U test), no other differences in PEWS were seen. Conclusions SARS-CoV-2 caused major changes in the incidence of paediatric respiratory viral infection in Oxfordshire, with implications for clinical service demand, testing strategies, timing of palivizumab RSV prophylaxis, and highlighting the need to understand which public health interventions are most effective for preventing respiratory virus infections.
Keywords: Influenza; Paediatric; Respiratory syncytial virus; Respiratory tract infection; Respiratory virus; Rhinovirus; SARS-CoV-2.
Copyright © 2021. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest DWE declares lecture fees from Gilead, outside the submitted work. No other author has a conflict of interest to declare.
Figures
References
-
- Couriel J. Assessment of the child with recurrent chest infections. Br Med Bull. 2002;61:115–132. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
