

Dexamethasone 12 mg versus 6 mg for patients with COVID-19 and severe hypoxaemia: a pre-planned, secondary Bayesian analysis of the COVID STEROID 2 trial
- PMID: 34757439
- PMCID: PMC8579417
- DOI: 10.1007/s00134-021-06573-1
Dexamethasone 12 mg versus 6 mg for patients with COVID-19 and severe hypoxaemia: a pre-planned, secondary Bayesian analysis of the COVID STEROID 2 trial
Abstract
Purpose: We compared dexamethasone 12 versus 6 mg daily for up to 10 days in patients with coronavirus disease 2019 (COVID-19) and severe hypoxaemia in the international, randomised, blinded COVID STEROID 2 trial. In the primary, conventional analyses, the predefined statistical significance thresholds were not reached. We conducted a pre-planned Bayesian analysis to facilitate probabilistic interpretation.
Methods: We analysed outcome data within 90 days in the intention-to-treat population (data available in 967 to 982 patients) using Bayesian models with various sensitivity analyses. Results are presented as median posterior probabilities with 95% credible intervals (CrIs) and probabilities of different effect sizes with 12 mg dexamethasone.
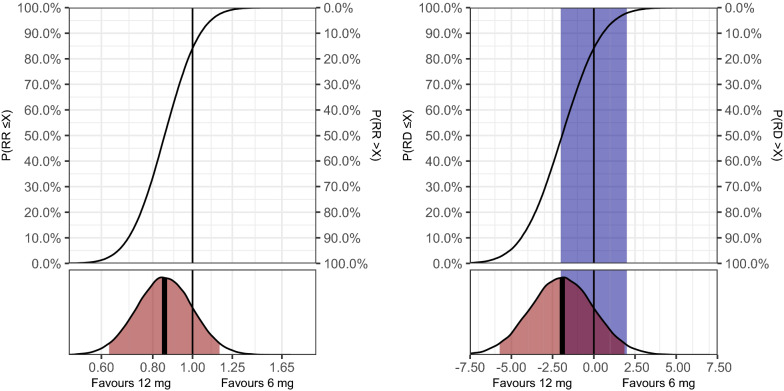
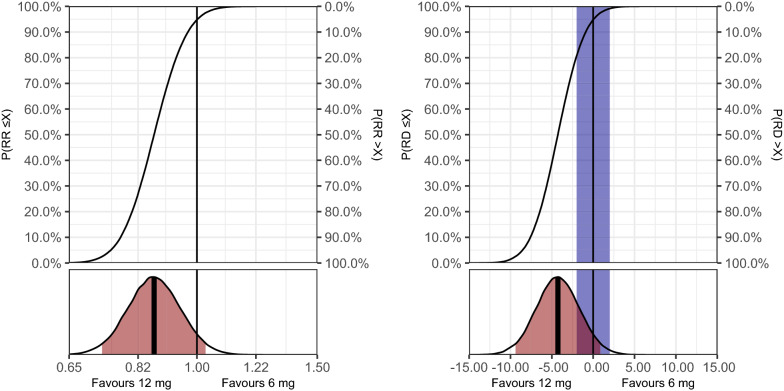
Results: The adjusted mean difference on days alive without life support at day 28 (primary outcome) was 1.3 days (95% CrI -0.3 to 2.9; 94.2% probability of benefit). Adjusted relative risks and probabilities of benefit on serious adverse reactions was 0.85 (0.63 to 1.16; 84.1%) and on mortality 0.87 (0.73 to 1.03; 94.8%) at day 28 and 0.88 (0.75 to 1.02; 95.1%) at day 90. Probabilities of benefit on days alive without life support and days alive out of hospital at day 90 were 85 and 95.7%, respectively. Results were largely consistent across sensitivity analyses, with relatively low probabilities of clinically important harm with 12 mg on all outcomes in all analyses.
Conclusion: We found high probabilities of benefit and low probabilities of clinically important harm with dexamethasone 12 mg versus 6 mg daily in patients with COVID-19 and severe hypoxaemia on all outcomes up to 90 days.
Trial registration: ClinicalTrials.gov NCT04509973.
Keywords: Bayesian analysis; COVID-19; Corticosteroids; Critical illness; Hypoxaemia.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
AG, MWM, MBNK, GKV, TSM, MHM and AP are affiliated with the Department of Intensive Care at Rigshospitalet, University of Copenhagen, which has received grants from the Novo Nordisk Foundation during the conduct of the trial; and grants from Pfizer, Fresenius Kabi, The Novo Nordisk Foundation, and Sygeforsikringen “danmark” outside the submitted work. SMJ and LC are affiliated with Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland, which has received grants from Edwards Lifesciences Services GmbH, Phagenesis Limited, and Nestlé; all outside the submitted work. TB has received grants from the Novo Nordisk Foundation, Simonsen Foundation, Lundbeck Foundation, Kai Hansen Foundation, and Erik and Susanna Olesen’s Charitable Fund; grants and personal fees from GSK, Pfizer, and Gilead; personal fees from Boehringer Ingelheim, MSD, and Pentabase ApS; all outside the submitted work. BV and NEH have received grants from Baxter outside the submitted work. VJ has received grants and personal fees from Baxter Healthcare; personal fees from Astra Zeneca, Visterra, Chinook, and NephroPlus; all outside the submitted work. CSU has received grants and personal fees from GSK, Sanofi Genzyme, Astra Zeneca, Teva, OrionPharma, Boehringer-Ingelheim, Actelion and Chiesi; grants, personal fees and non-financial support from Novartis; all outside the submitted work.JVD has received personal fees (paid to his institution) from Edwards India outside the submitted work. PA has received personal fees from CIPLA, Dr. Reddy’s Laboratories, Abbott Nutrition and Sanofi; all outside the submitted work. The remaining authors declared no known conflicts of interest.
Figures

Comment in
-
Pick your prior: scepticism about sceptical prior beliefs.Intensive Care Med. 2022 Mar;48(3):374-375. doi: 10.1007/s00134-021-06602-z. Epub 2021 Dec 17. Intensive Care Med. 2022. PMID: 34919155 Free PMC article. No abstract available.
-
Choice of priors: how much scepticism is appropriate?Intensive Care Med. 2022 Mar;48(3):372-373. doi: 10.1007/s00134-021-06613-w. Epub 2022 Jan 13. Intensive Care Med. 2022. PMID: 35024884 No abstract available.
References
-
- World Health Organization (2021) Coronavirus disease (COVID-19) Pandemic. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed 27 Sep 2021.
-
- Rochwerg B, Agarwal A, Siemieniuk RA, et al. A living WHO guideline on drugs for covid-19. BMJ. 2020;370:m3379. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
