

US emergency department visits for acute harms from over-the-counter cough and cold medications, 2017-2019
- PMID: 34757641
- PMCID: PMC10917081
- DOI: 10.1002/pds.5384
US emergency department visits for acute harms from over-the-counter cough and cold medications, 2017-2019
Abstract
Background and purpose: Characterization of emergency department (ED) visits for acute harms related to use of over-the-counter cough and cold medications (CCMs) by patient demographics, intent of CCM use, concurrent substance use, and clinical manifestations can help guide prevention of medication harms.
Methods: Public health surveillance data from the National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance project were used to estimate numbers and population rates of ED visits from 2017 to 2019.
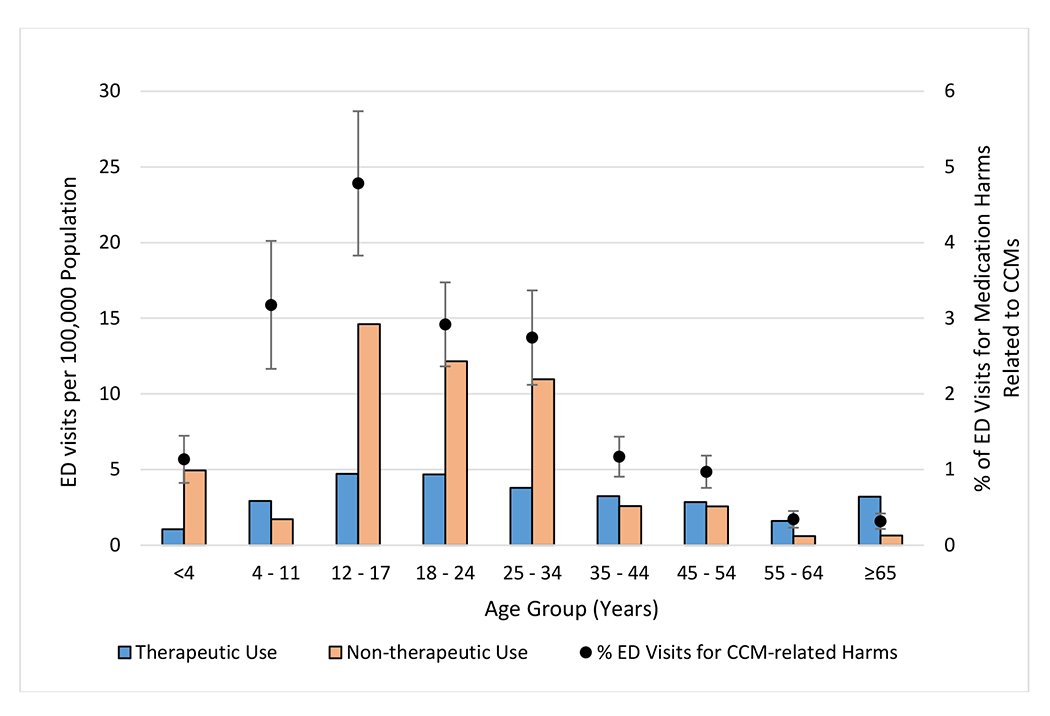
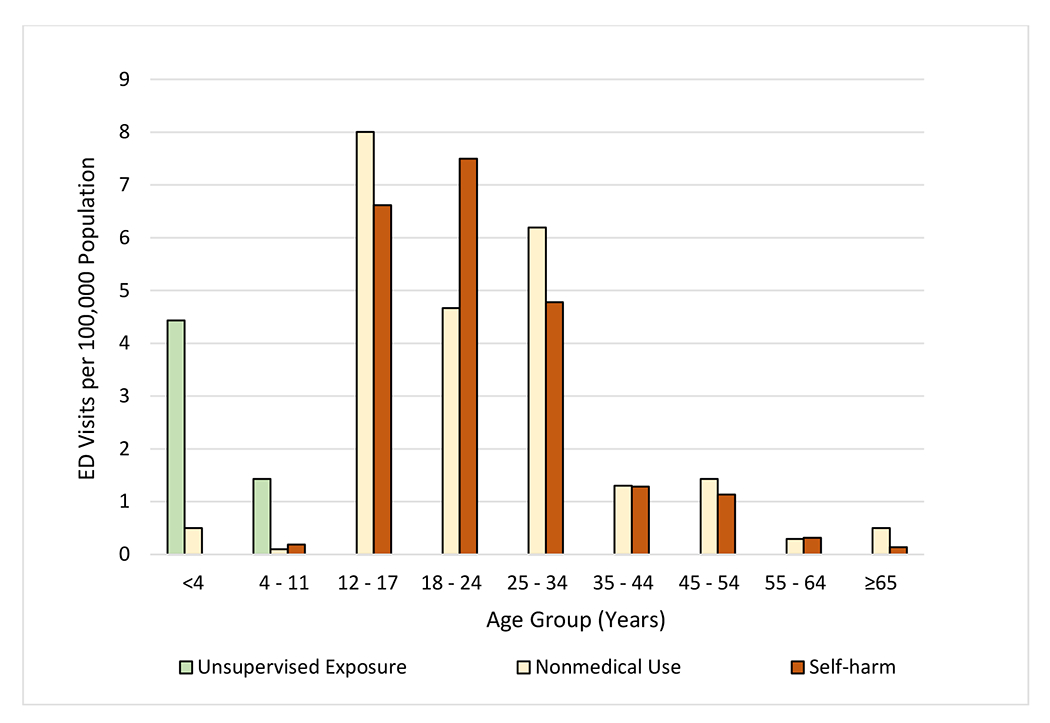
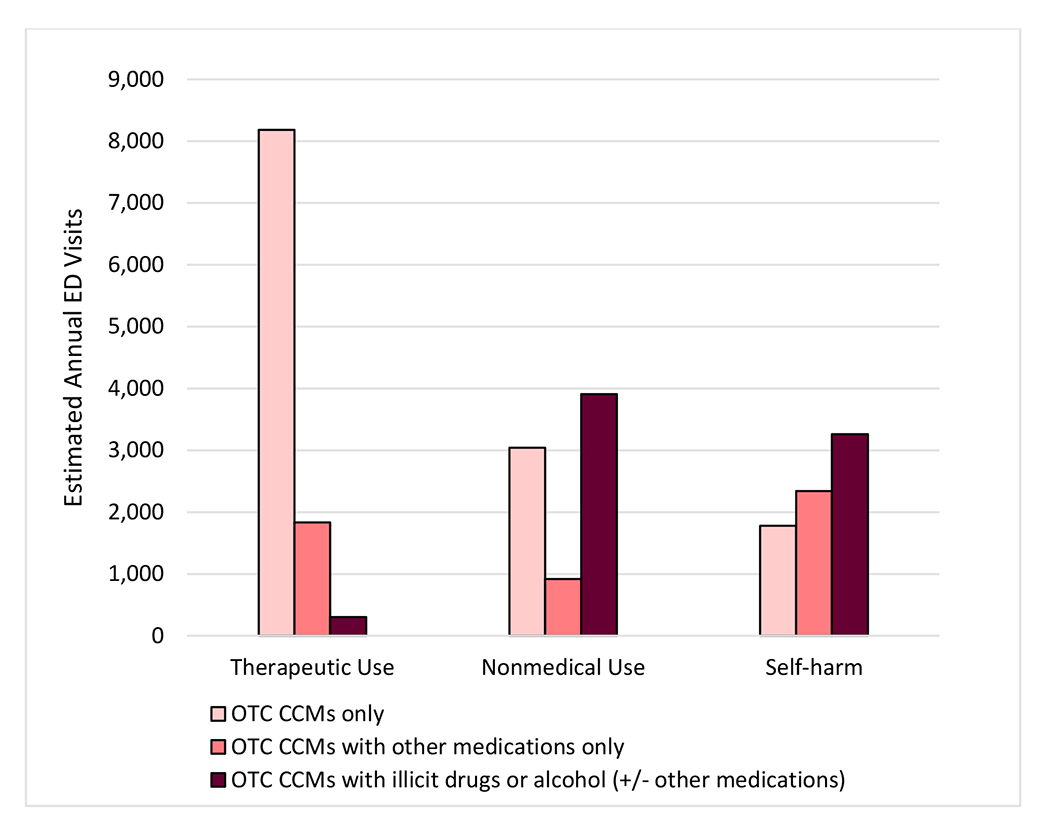
Results: Based on 1396 surveillance cases, there were an estimated 26 735 (95% CI, 21 679-31 791) US ED visits for CCM-related harms annually, accounting for 1.3% (95% CI, 1.2-1.5%) of all ED visits for medication adverse events. Three fifths (61.4%, 95% CI, 55.6-67.2%) of these visits were attributed to non-therapeutic CCM use (nonmedical use, self-harm, unsupervised pediatric exposures). Most visits by children aged <4 years (74.0%, 95% CI, 59.7-88.3%) were for unsupervised CCM exposures. Proportion hospitalized was higher for visits for self-harm (76.5%, 95% CI, 68.9-84.2%) than for visits for nonmedical use (30.3%, 95% CI, 21.1-39.6%) and therapeutic use (8.8%, 95% CI, 5.9-11.8%). Overall, estimated population rates of ED visits for CCM-related harms were higher for patients aged 12-34 years (16.5 per 100 000, 95% CI, 13.0-20.0) compared with patients aged <12 years (5.1 per 100 000, 95% CI, 3.6-6.5) and ≥ 35 years (4.3 per 100 000, 95% CI, 3.4-5.1). Concurrent use of other medications, illicit drugs, or alcohol was frequent in ED visits for nonmedical use (61.3%) and self-harm (75.9%).
Conclusions: Continued national surveillance of CCM-related harms can assess progress toward safer use.
Keywords: adverse drug event; cough and cold medication; medication safety; nonmedical drug use; unsupervised exposure.
Published 2021. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
Figures
References
-
- Fashner J, Ericson K, Werner S. Treatment of the common cold in children and adults. Am Fam Physician 2012;86(2):153–9. - PubMed
-
- Consumer Healthcare Products Association. OTC Use Statistics. https://www.chpa.org/about-consumer-healthcare/research-data/otc-use-sta.... Published 2019. Accessed July 13, 2021.
-
- US Department of Health and Human Services, National Institutes of Health, National Library of Medicine. Cough and Cold Medicines. MedLinePlus. https://medlineplus.gov/coldandcoughmedicines.html. Published 2021. Accessed June 21, 2021.
-
- Green JL, Wang GS, Reynolds KM, et al. Safety Profile of Cough and Cold Medication Use in Pediatrics. Pediatrics 2017;139(6). - PubMed
-
- Chyka PA, Erdman AR, Manoguerra AS, et al. Dextromethorphan poisoning: an evidence-based consensus guideline for out-of-hospital management. Clin Toxicol (Phila) 2007;45(6):662–77. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
