

Pulmonary tumor thrombotic microangiopathy in occult early gastric cancer that was undetectable on upper endoscopy: a case report and review of similar cases
- PMID: 34758740
- PMCID: PMC8579618
- DOI: 10.1186/s12876-021-02009-8
Pulmonary tumor thrombotic microangiopathy in occult early gastric cancer that was undetectable on upper endoscopy: a case report and review of similar cases
Abstract
Background: Pulmonary tumor thrombotic microangiopathy (PTTM), a rare manifestation of metastatic cancer with poor prognosis, is characterized by subacute/acute fatal pulmonary hypertension. The main cause of PTTM is gastric cancer, and cases of early gastric cancer confirmed using autopsy have been reported. Moreover, several cases of early gastric cancer that are undetectable on endoscopy or macroscopic postmortem examination have been reported.
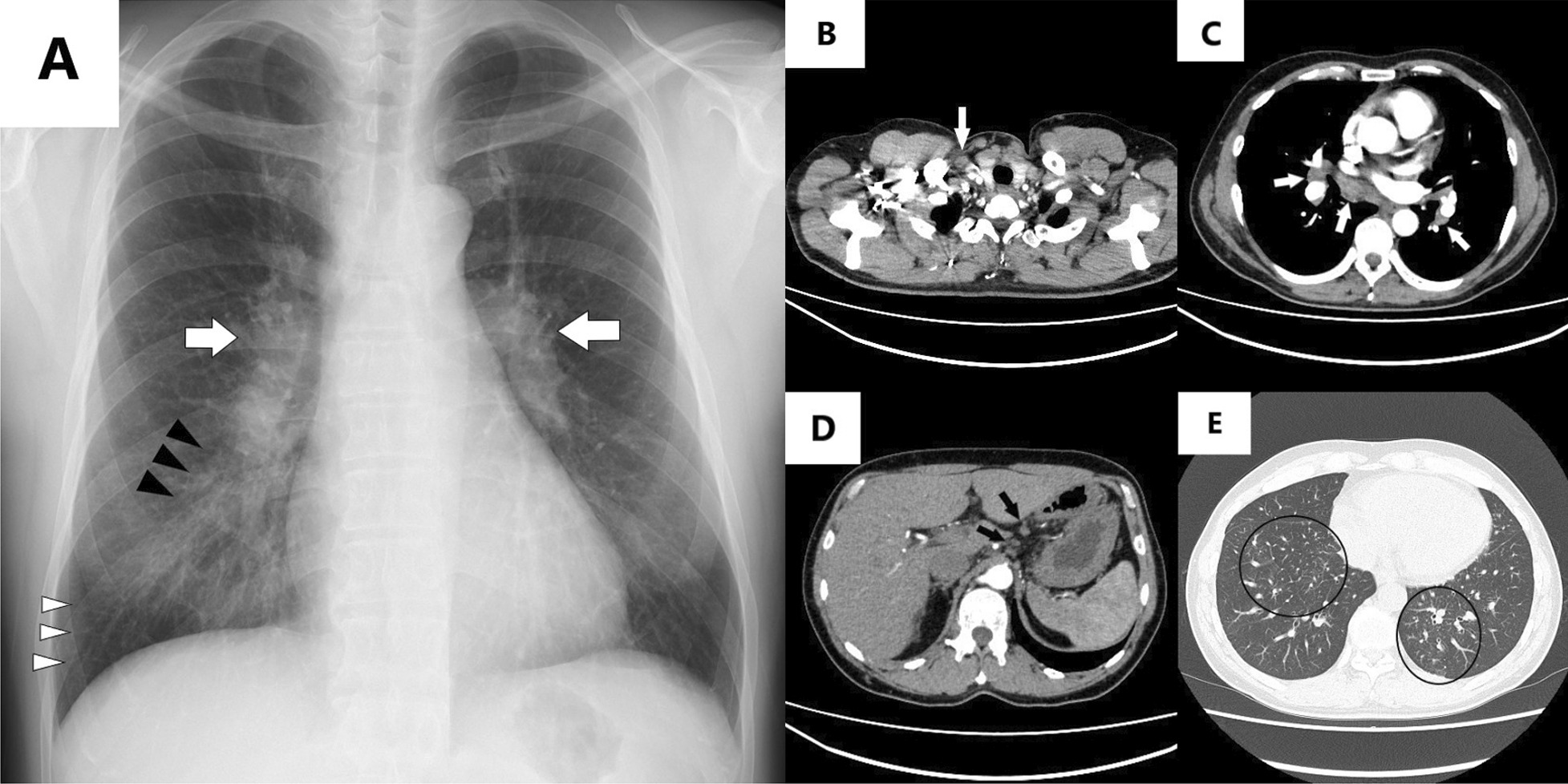
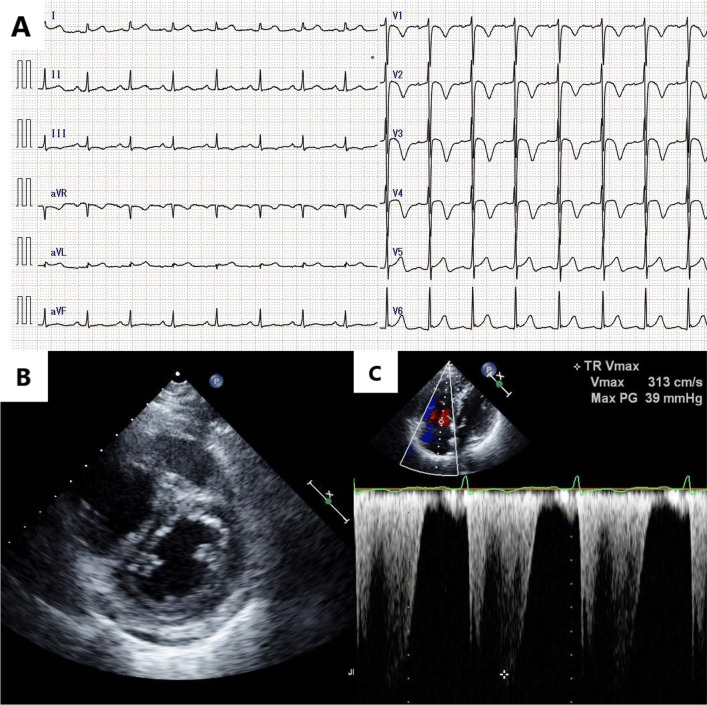
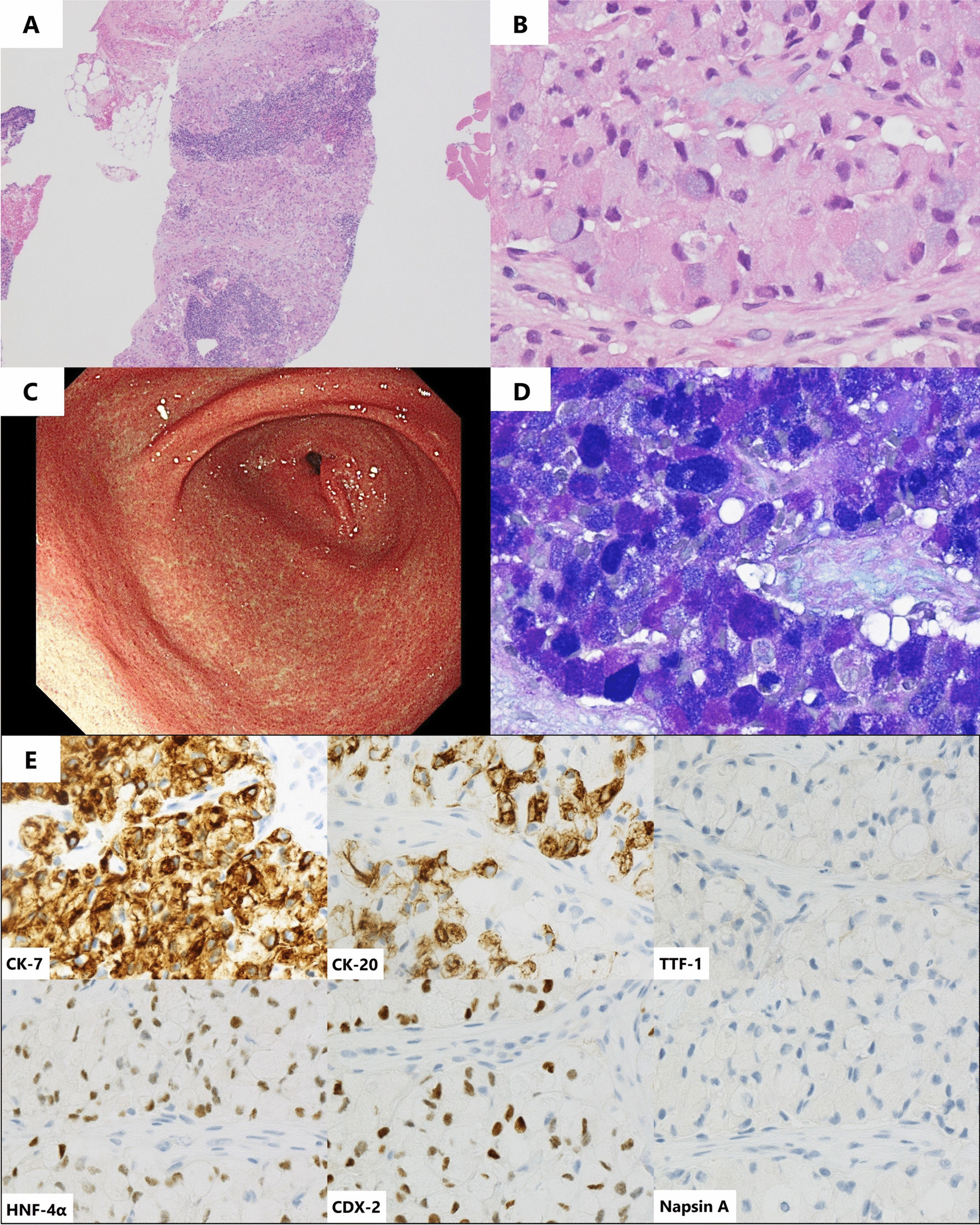
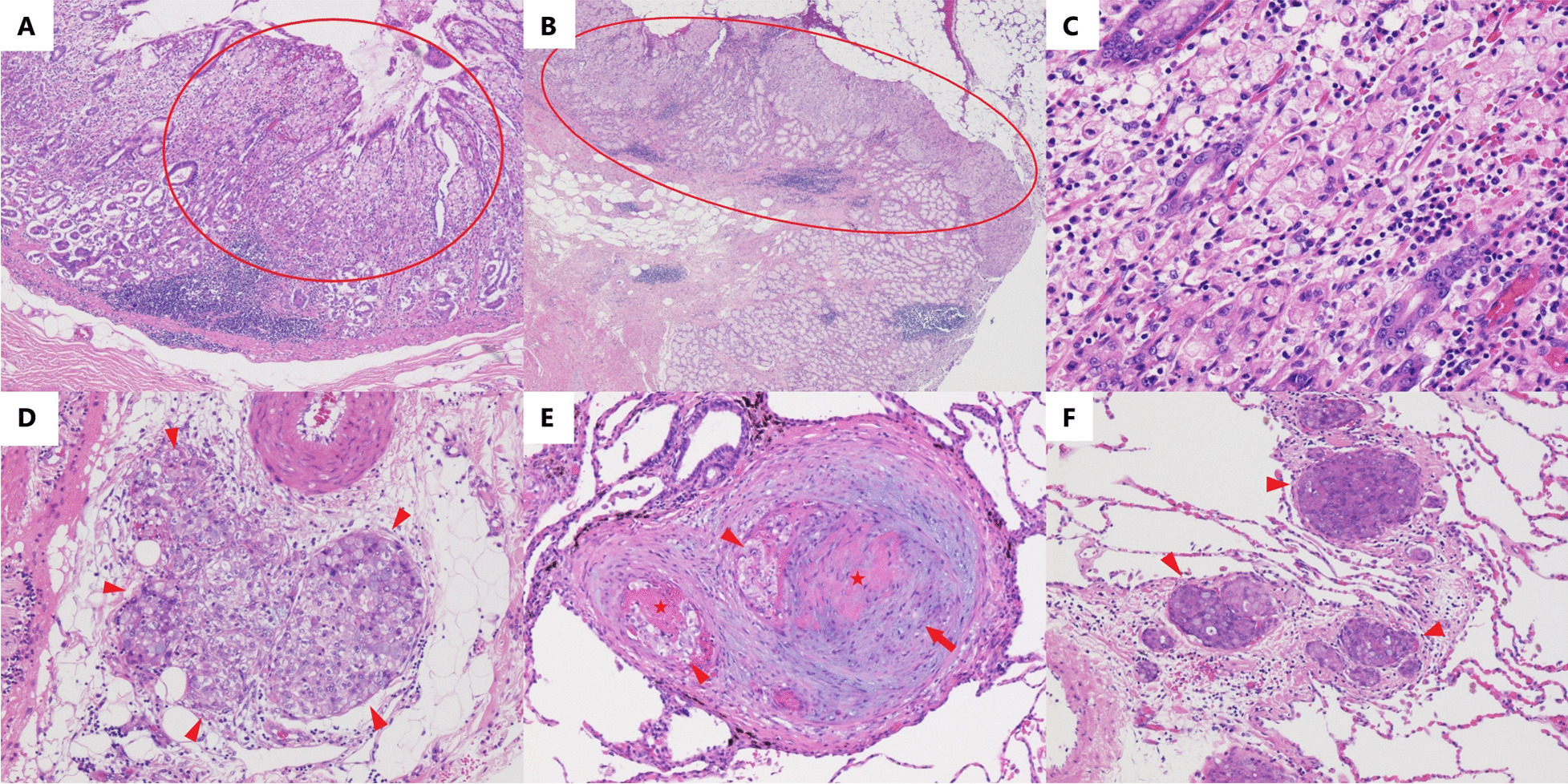
Case presentation: A previously healthy 50-year-old man presented with progressive dyspnea and cough for 1 month. Echocardiography suggested pulmonary hypertension. Computed tomography revealed diffuse lymphadenopathy, whereas blood work revealed an elevation in several serum tumor marker levels. Despite normal upper endoscopic findings, a presumptive diagnosis of PTTM due to gastric cancer was made based on pathological findings of cervical lymph node biopsy, which indicated signet ring cell carcinoma. Imatinib and tegafur/gimeracil/oteracil plus oxaliplatin therapy were started on day 7. The patient's condition was initially stable. However, his symptoms suddenly progressed, and the patient died on day 8. Macroscopic postmortem examination revealed no abnormal gastric wall findings. Microscopically, PTTM was confirmed, and multiple serial sections of the stomach revealed early gastric cancer.
Conclusions: Despite normal endoscopic findings, micro-occult gastric cancer can lead to PTTM. Physicians should be aware of this disease presentation. Taking prompt action is needed when PTTM is suspected, even if the patient appears stable.
Keywords: Early gastric cancer; Endoscopy; Imatinib; Pulmonary tumor thrombotic microangiopathy; Signet ring cell carcinoma.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that there is no competing interests regarding the publication of this article.
Figures
References
-
- Igarashi S, Kawaguchi T, Hoshi N. Early gastric cancer carcinoma with widespread metastasis and pulmonary tumor thrombotic microangiopathy (PTTM): report of an autopsy case. I to Cho (Stomach Intest) 1997;32:861–865.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
