

Sonography of diffuse thyroid disease
- PMID: 34760439
- PMCID: PMC8409448
- DOI: 10.1002/ajum.12001
Sonography of diffuse thyroid disease
Abstract
Introduction/purpose: This article aims to review of the common diffuse thyroid disease.
Methods: Thorough literature search and review was performed for each diffuse thyroid disease. The most recent and updated ultrasound images were obtained.
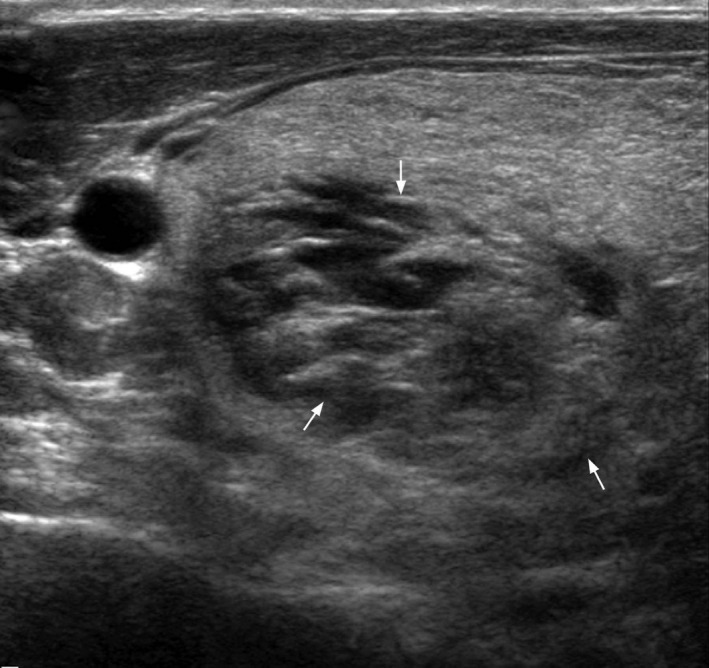
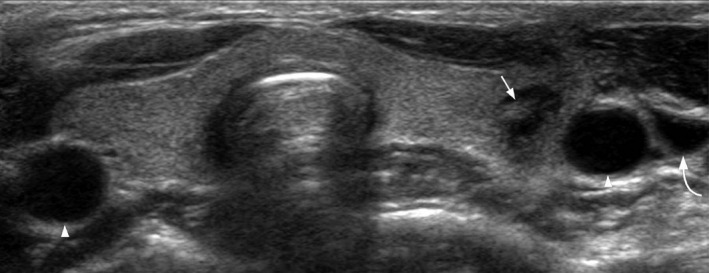
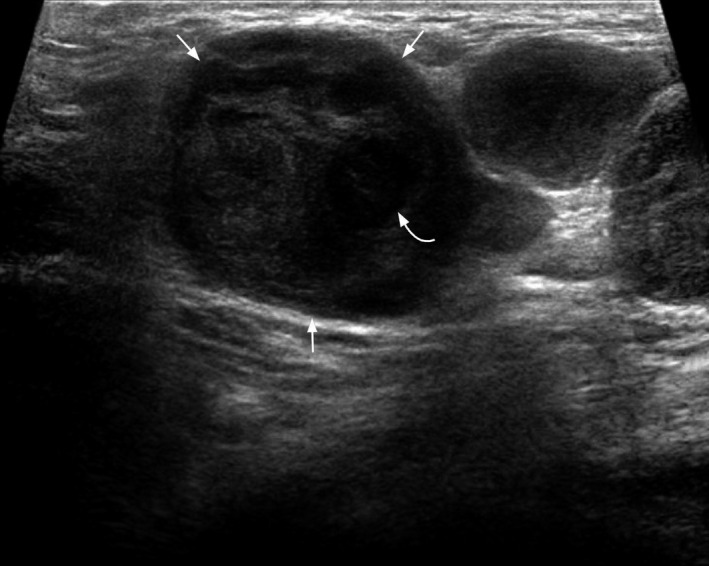
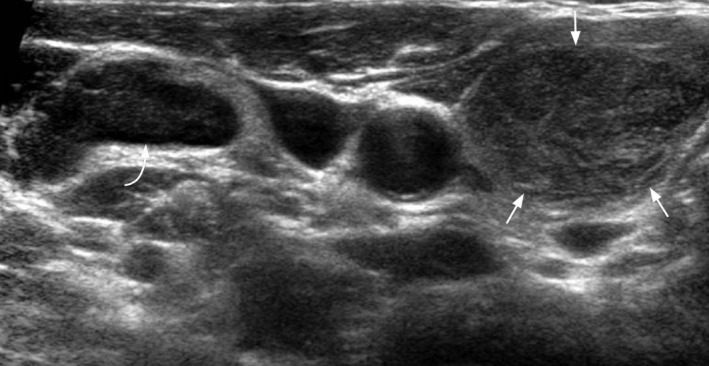
Results: Diffuse thyroid diseases discussed include multinodular goitre, Graves' disease, Hashimoto thyroiditis, de Quervain thyroiditis, acute suppurative thyroiditis, anaplastic carcinoma, thyroid metastases, chronic lymphocytic leukaemia/small lymphocytic lymphoma, Langerhans cell histiocytosis, tuberculosis, plasmacytoma, IgG4-related disease and thyrolipoma.
Discussion: The major clinical features and the sonographic features of each diffuse thyroid disease are reviewed.
Conclusion: This article serves as a synopsis of diffuse thyroid disease.
Keywords: diffuse thyroid disease; ultrasound.
© 2016 Australasian Society for Ultrasound in Medicine.
Figures















Similar articles
-
Likelihood ratio-based differentiation of nodular Hashimoto thyroiditis and papillary thyroid carcinoma in patients with sonographically evident diffuse hashimoto thyroiditis: preliminary study.J Ultrasound Med. 2012 Nov;31(11):1767-75. doi: 10.7863/jum.2012.31.11.1767. J Ultrasound Med. 2012. PMID: 23091247
-
The usefulness of conventional and echo colour Doppler sonography in the differential diagnosis of toxic multinodular goitres.Eur J Endocrinol. 2000 Sep;143(3):339-46. doi: 10.1530/eje.0.1430339. Eur J Endocrinol. 2000. PMID: 11022175 Clinical Trial.
-
Thyroid Ultrasonography in Differentiation between Graves' Disease and Hashimoto's Thyroiditis.J Biomed Phys Eng. 2017 Mar 1;7(1):21-26. eCollection 2017 Mar. J Biomed Phys Eng. 2017. PMID: 28451576 Free PMC article.
-
[Sonography of the thyroid].Praxis (Bern 1994). 2006 Apr 12;95(15):575-80. doi: 10.1024/0369-8394.95.15.575. Praxis (Bern 1994). 2006. PMID: 16640177 Review. German.
-
Development of Graves' Disease After SARS-CoV-2 mRNA Vaccination: A Case Report and Literature Review.Front Public Health. 2021 Nov 23;9:778964. doi: 10.3389/fpubh.2021.778964. eCollection 2021. Front Public Health. 2021. PMID: 34888290 Free PMC article. Review.
Cited by
-
Visualizing thyroid health: a pictorial journey through 2017 ACR TI-RADS and common thyroid pathologies.Ann Med Surg (Lond). 2024 Jul 23;86(9):5377-5388. doi: 10.1097/MS9.0000000000002398. eCollection 2024 Sep. Ann Med Surg (Lond). 2024. PMID: 39239024 Free PMC article. Review.
-
Primary thyroid tuberculosis mimicking papillary carcinoma of thyroid: a rare case report.Ann Med Surg (Lond). 2023 Apr 11;85(5):2155-2158. doi: 10.1097/MS9.0000000000000648. eCollection 2023 May. Ann Med Surg (Lond). 2023. PMID: 37228911 Free PMC article.
-
The relationship between ultrasound findings and thyroid function in children and adolescent autoimmune diffuse thyroid diseases.Sci Rep. 2021 Oct 5;11(1):19709. doi: 10.1038/s41598-021-99016-2. Sci Rep. 2021. PMID: 34611214 Free PMC article.
-
Diagnostic Tools Applied to Determine Thyroid Lipoadenoma: A Case Report.Cureus. 2025 Apr 27;17(4):e83096. doi: 10.7759/cureus.83096. eCollection 2025 Apr. Cureus. 2025. PMID: 40438843 Free PMC article.
-
Acute suppurative thyroiditis in a child with congenital third/fourth branchial arch anomaly: a case report.Pan Afr Med J. 2024 Jul 19;48:120. doi: 10.11604/pamj.2024.48.120.38164. eCollection 2024. Pan Afr Med J. 2024. PMID: 39545034 Free PMC article.
References
-
- Levy MJ, Howlett TA. Endocrine disease. In: Kumar P, Clark M, et al., editors. Kumar & Clark's clinical medicine. 8th edn. Spain: Saunders Elsevier; 2012. 959–71.
-
- Baumann GP, Jameson JL. Thyroid gland disorders. In: Longo DL, et al., editors. Harrison's manual of medicine, 18th edn. USA: McGraw Hill; 2013. 1116–26.
-
- Maitra A. The endocrine system. In: Kumar V, Abbas AK, Aster JC, et al., editors. Robbins and Cotran pathological basis of disease, 9th edn. Canada: Elsevier Saunders; 2015. 1091–2.
-
- Ahuja AT, Lee YYP, Wong KT. Multinodular goiter. In: Ahuja AT, et al., editors. Diagnostic ultrasound: head and neck, Vol. II‐2. Altona, MB: Friesens; 2014. 22–5.
LinkOut - more resources
Full Text Sources