

Clinical features and mortality in COVID-19 SARI versus non COVID-19 SARI cases from Western Rajasthan, India
- PMID: 34760737
- PMCID: PMC8565113
- DOI: 10.4103/jfmpc.jfmpc_14_21
Clinical features and mortality in COVID-19 SARI versus non COVID-19 SARI cases from Western Rajasthan, India
Abstract
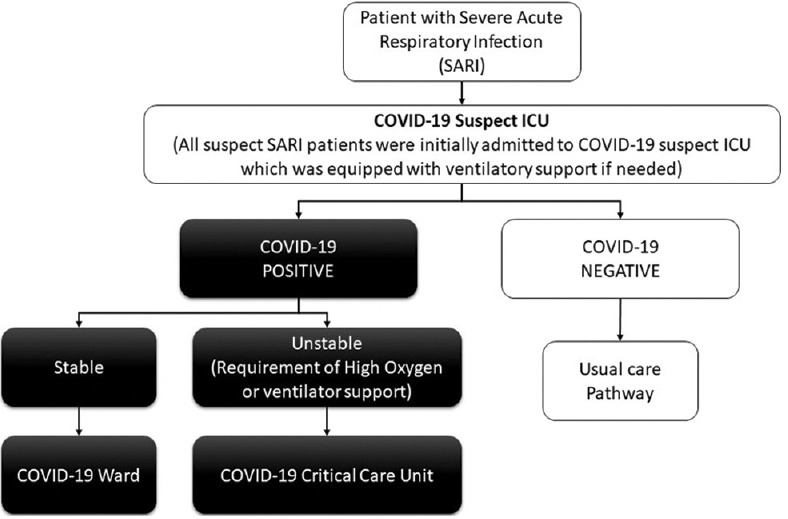
Background: In March 2020, the Indian Council of Medical Research (ICMR) issued guidelines that all patients presenting with severe acute respiratory infections (SARI) should be investigated for coronavirus disease 2019 (COVID-19). Following the same protocol, in our institute, all patients with SARI were transferred to the COVID-19 suspect intensive care unit (ICU) and investigated for COVID-19.
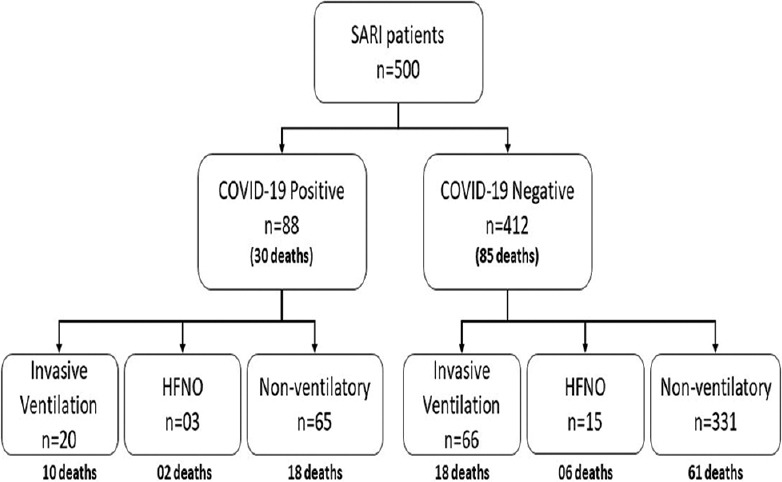
Methods: This study was planned to examine the demographical, clinical features, and outcomes of the first 500 suspected patients of COVID-19 with SARI admitted in the COVID-19 suspect ICU at a tertiary care center. Between March 7 and July 20, 2020, 500 patients were admitted to the COVID-19 suspect ICU. We analyzed the demographical, clinical features, and outcomes between COVID-19 positive and negative SARI cases. The records of all the patients were reviewed until July 31, 2020.
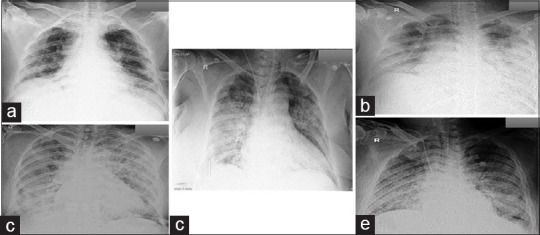
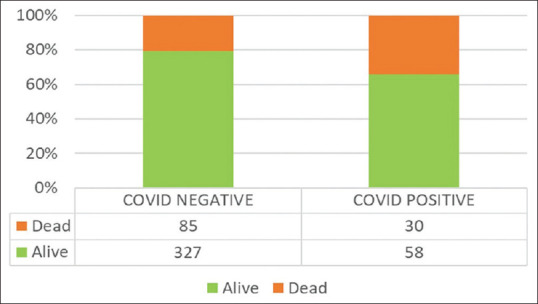
Results: Of the 500 suspected patients admitted to the hospital, 88 patients showed positive results for COVID-19 by reverse transcription-polymerase chain reaction (RT-PCR) of the nasopharyngeal swabs. The mean age in the positive group was higher (55.31 ± 16.16 years) than in the negative group (40.46 ± 17.49 years) (P < 0.001). Forty-seven (53.4%) of these patients in the COVID-19 positive group and 217 (52.7%) from the negative group suffered from previously known comorbidities. The common symptoms included fever, cough, sore throat, and dyspnea. Eighty-five (20.6%) patients died in the COVID-19 negative group, and 30 (34.1%) died in the COVID-19 positive group (P = 0.006). Deaths among the COVID-19 positive group had a significantly higher age than deaths in the COVID-19 negative group (P < 0.001). Among the patients who died with positive COVID-19 status had substantially higher neutrophilia and lymphopenia (P < 0.001). X-ray chest abnormalities were almost three times more likely in COVID-19 deaths (P < 0.001).
Conclusion: In the present article, 17.6% of SARI were due to COVID-19 infection with significantly higher mortality (34.1%) in COVID-19 positive patients with SARI. Although all patients presenting as SARI have considerable mortality rates, the COVID-19-associated SARI cases thus had an almost one-third risk of mortality.
Keywords: Coronavirus Disease 2019; SARS-CoV2; severe acute respiratory infection.
Copyright: © 2021 Journal of Family Medicine and Primary Care.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Clinical Profile and Outcome of Severe Acute Respiratory Illness (SARI) in Children Amidst the COVID-19 Pandemic.Cureus. 2024 Jun 7;16(6):e61902. doi: 10.7759/cureus.61902. eCollection 2024 Jun. Cureus. 2024. PMID: 38978920 Free PMC article.
-
Clinical and Epidemiological Features of SARS-CoV-2 Patients in SARI Ward of a Tertiary Care Centre in New Delhi.J Assoc Physicians India. 2020 Jul;68(7):19-26. J Assoc Physicians India. 2020. PMID: 32602676
-
COVID-19 Pandemic: Impact on Admission, Diagnosis, and Treatment of Non-COVID-19 Patients Admitted to SARI ICU.Indian J Crit Care Med. 2021 Aug;25(8):853-859. doi: 10.5005/jp-journals-10071-23942. Indian J Crit Care Med. 2021. PMID: 34733023 Free PMC article.
-
Severe Acute Respiratory Infection Surveillance during the Initial Phase of the COVID-19 Outbreak in North India: A Comparison of COVID-19 to Other SARI Causes.Indian J Crit Care Med. 2021 Jul;25(7):761-767. doi: 10.5005/jp-journals-10071-23882. Indian J Crit Care Med. 2021. PMID: 34316169 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
Cited by
-
Clinical Profile and Outcome of Severe Acute Respiratory Illness (SARI) in Children Amidst the COVID-19 Pandemic.Cureus. 2024 Jun 7;16(6):e61902. doi: 10.7759/cureus.61902. eCollection 2024 Jun. Cureus. 2024. PMID: 38978920 Free PMC article.
-
Clinical and epidemiological aspects of severe acute respiratory infection: before and during the first year of the COVID-19 pandemic in Brazil.Trans R Soc Trop Med Hyg. 2023 Mar 1;117(3):161-173. doi: 10.1093/trstmh/trac074. Trans R Soc Trop Med Hyg. 2023. PMID: 35929810 Free PMC article.
-
Incidence of common respiratory pathogens among patients with severe acute respiratory infection during COVID-19 pandemic in Egypt.Sci Rep. 2025 May 5;15(1):15711. doi: 10.1038/s41598-025-98907-y. Sci Rep. 2025. PMID: 40325147 Free PMC article.
-
Dichotomous outcomes vs. survival regression models for identification of predictors of mortality among patients with severe acute respiratory illness during COVID-19 pandemics.Front Public Health. 2023 Dec 6;11:1271177. doi: 10.3389/fpubh.2023.1271177. eCollection 2023. Front Public Health. 2023. PMID: 38125848 Free PMC article.
-
Characterizing deaths among adult patients with severe acute respiratory infection: during the pre- and COVID-19 pandemic periods in Bangladesh, 2018-2022.Trop Med Health. 2023 Dec 19;51(1):70. doi: 10.1186/s41182-023-00565-1. Trop Med Health. 2023. PMID: 38115037 Free PMC article.
References
-
- Sahu KK, Mishra AK, Lal A. COVID-2019: Update on epidemiology, disease spread, and management. Monaldi Arch Chest Dis. 2020:90. doi: 10.4081/monaldi. 2020.1292. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous