

Deciphering glial scar after spinal cord injury
- PMID: 34761050
- PMCID: PMC8576268
- DOI: 10.1093/burnst/tkab035
Deciphering glial scar after spinal cord injury
Abstract
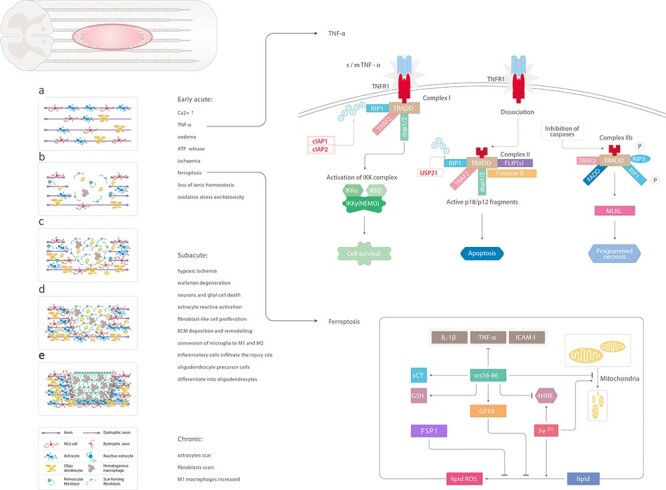
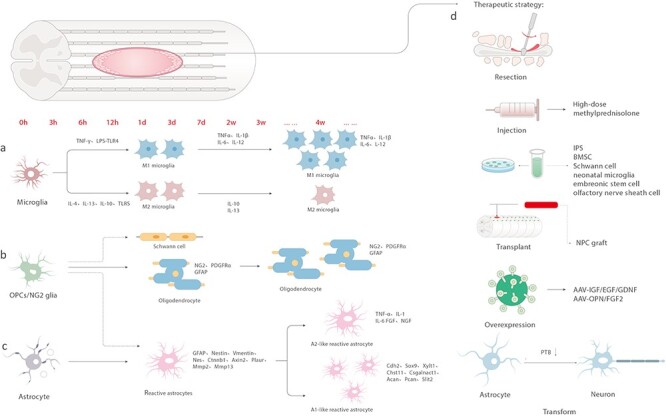
Spinal cord injury (SCI) often leads to permanent disability, which is mainly caused by the loss of functional recovery. In this review, we aimed to investigate why the healing process is interrupted. One of the reasons for this interruption is the formation of a glial scar around the severely damaged tissue, which is usually covered by reactive glia, macrophages and fibroblasts. Aiming to clarify this issue, we summarize the latest research findings pertaining to scar formation, tissue repair, and the divergent roles of blood-derived monocytes/macrophages, ependymal cells, fibroblasts, microglia, oligodendrocyte progenitor cells (OPCs), neuron-glial antigen 2 (NG2) and astrocytes during the process of scar formation, and further analyse the contribution of these cells to scar formation. In addition, we recapitulate the development of therapeutic treatments targeting glial scar components. Altogether, we aim to present a comprehensive decoding of the glial scar and explore potential therapeutic strategies for improving functional recovery after SCI.
Keywords: Axon regeneration; Glial scar; Spinal cord injury; Therapeutic strategy.
© The Author(s) 2021. Published by Oxford University Press.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
