

Evaluating the association of frailty with communication about aging-related concerns between older patients with advanced cancer and their oncologists
- PMID: 34762734
- PMCID: PMC8837685
- DOI: 10.1002/cncr.34010
Evaluating the association of frailty with communication about aging-related concerns between older patients with advanced cancer and their oncologists
Abstract
Background: A geriatric assessment (GA) intervention improves communication about aging-related concerns, but its effect on communication in patients with various levels of frailty is unknown.
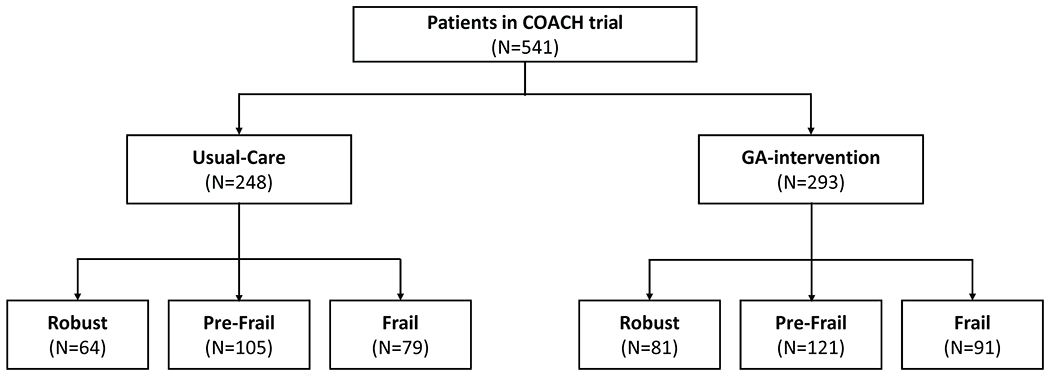
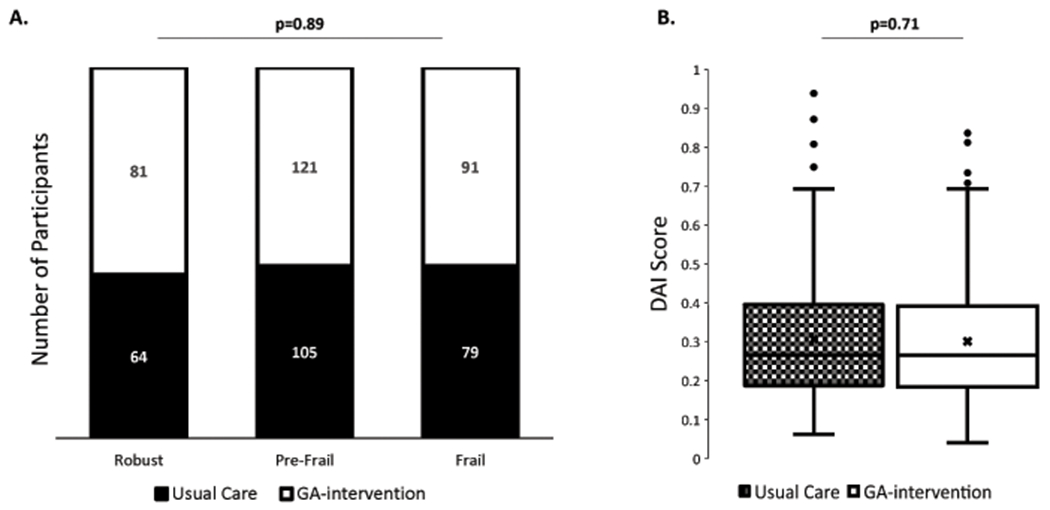
Methods: This was a secondary analysis of a nationwide trial of patients aged ≥70 years with incurable cancer and impairment on 1 or more GA domains (ClinicalTrials.gov Identifier NCT02107443; principal investigator Supriya G. Mohile). Practice sites were randomized to either the GA-intervention or usual care. Frailty was assessed with a deficit accumulation index (range, 0-1), and patients were stratified as robust (0 to <0.2), prefrail (0.2 to <0.35), or frail (≥0.35). The clinic visit after the GA-intervention was audio-recorded, transcribed, and coded to evaluate the number and quality of conversations about aging-related concerns. Linear mixed models examined differences in the number and quality of conversations within and between arms. All P values were 2-sided.
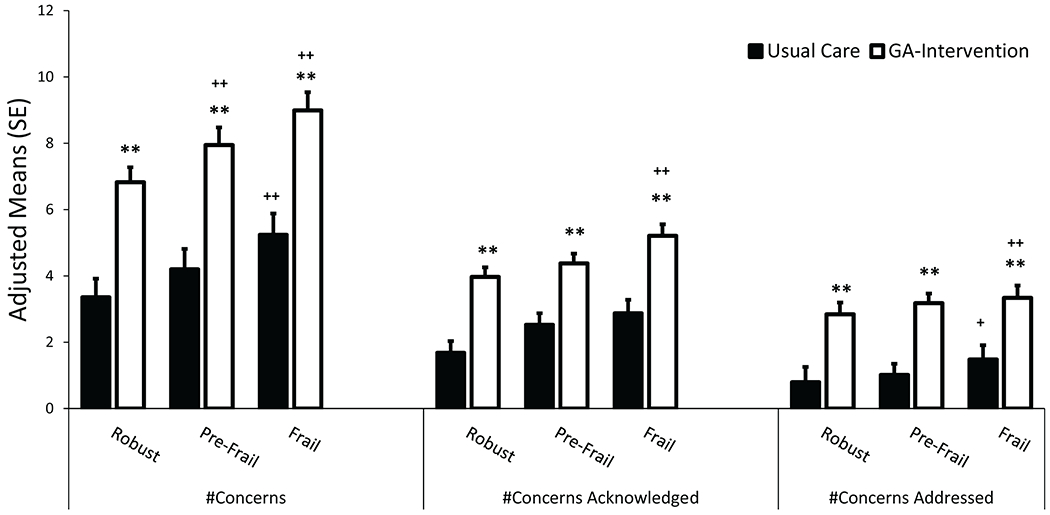
Results: Patients (n = 541) were classified as robust (27%), prefrail (42%), or frail (31%). In the usual care arm, frail patients (vs robust ones) engaged in more aging-related conversations (adjusted mean difference, 1.73; 95% confidence interval [CI], 0.59-2.87), conversations of higher quality (difference, 1.12; 95% CI, 0.24-2.0), and more discussions about evidence-based recommendations (difference, 0.71; 95% CI, 0.04-1.38; all P values ≤ .01). Similarly, in the GA intervention arm, frail patients (vs robust ones) engaged in more aging-related conversations (difference, 2.49; 95% CI, 1.51-3.47), conversations of higher quality (difference, 1.31; 95% CI, 0.56-2.06), and more discussions about evidence-based recommendations (difference, 0.87; 95% CI, 0.32-1.42; all P values ≤ .01). Furthermore, the GA-intervention significantly improved the number and quality of conversations in all patients: robust, prefrail, and frail (all P values ≤ .01).
Conclusions: Patients with higher degrees of frailty and those exposed to the GA-intervention had more and higher quality conversations about aging-related concerns with oncologists.
Lay summary: A geriatric assessment (GA) intervention improves communication about aging-related concerns, but its effect on communication in patients with various levels of frailty is unknown. This study conducted a secondary analysis of a nationwide trial of patients aged ≥70 years with incurable cancer and 1 or more GA domain impairments. Patients were stratified as robust, prefrail, or frail. The number and quality of conversations about aging-related concerns that occurred during the clinic visit after the GA-intervention were determined. Patients with higher degrees of frailty and those in the GA intervention arm had more and higher quality conversations about aging-related concerns with oncologists.
Keywords: communication; frailty; geriatric assessment; older adults with cancer; satisfaction with communication.
© 2021 American Cancer Society.
Conflict of interest statement
Figures
Comment in
-
Multidimensional impact of the geriatric assessment in the cancer care of older adults.Cancer. 2022 Mar 1;128(5):953-955. doi: 10.1002/cncr.34009. Epub 2021 Nov 11. Cancer. 2022. PMID: 34762733 No abstract available.
References
-
- Rockwood K, Howlett SE. Age-related deficit accumulation and the diseases of ageing. Mech Ageing Dev. 2019;180: 107–116. - PubMed
-
- Ethun CG, Bilen MA, Jani AB, Maithel SK, Ogan K, Master VA. Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA Cancer J Clin. 2017;67: 362–377. - PubMed
