

Integration of adeno-associated virus (AAV) into the genomes of most Thai and Mongolian liver cancer patients does not induce oncogenesis
- PMID: 34763675
- PMCID: PMC8588581
- DOI: 10.1186/s12864-021-08098-9
Integration of adeno-associated virus (AAV) into the genomes of most Thai and Mongolian liver cancer patients does not induce oncogenesis
Abstract
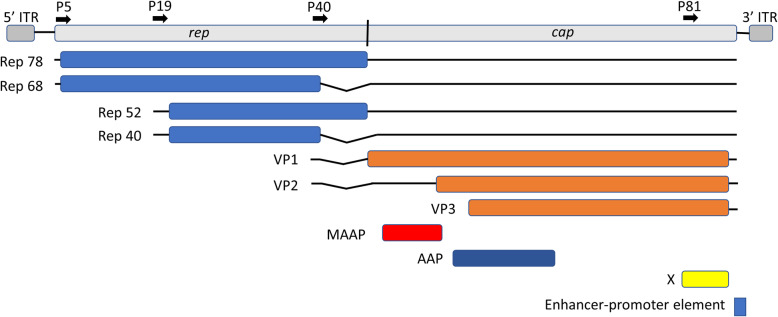
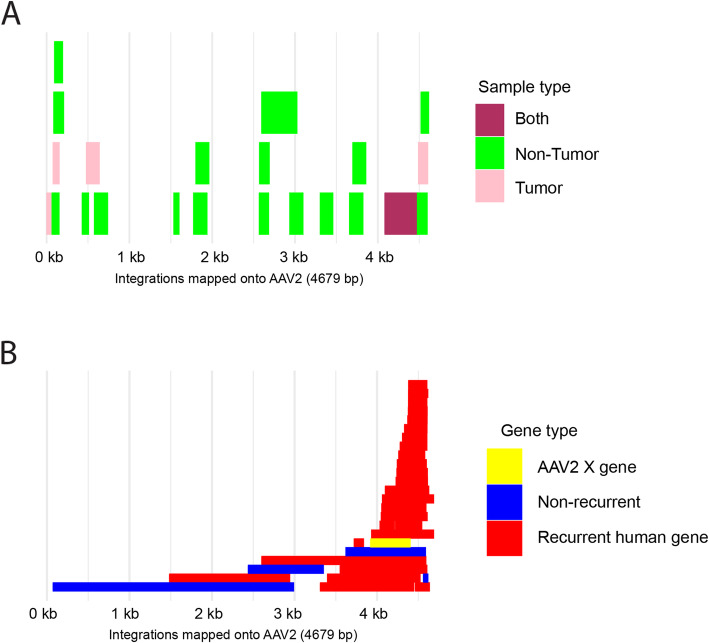
Background: Engineered versions of adeno-associated virus (AAV) are commonly used in gene therapy but evidence revealing a potential oncogenic role of natural AAV in hepatocellular carcinoma (HCC) has raised concerns. The frequency of potentially oncogenic integrations has been reported in only a few populations. AAV infection and host genome integration in another type of liver cancer, cholangiocarcinoma (CCA), has been studied only in one cohort. All reported oncogenic AAV integrations in HCC come from strains resembling the fully sequenced AAV2 and partly sequenced AAV13. When AAV integration occurs, only a fragment of the AAV genome is detectable in later DNA or RNA sequencing. The integrated fragment is typically from the 3' end of the AAV genome, and this positional bias has been only partly explained. Three research groups searched for evidence of AAV integration in HCC RNAseq samples in the Cancer Genome Atlas (TCGA) but reported conflicting results.
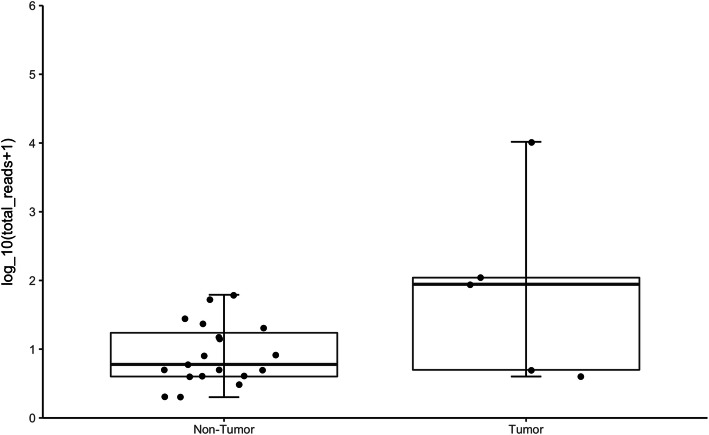
Results: We collected and analyzed whole transcriptome and viral capture DNA sequencing in paired tumor and non-tumor samples from two liver cancer Asian cohorts from Thailand (N = 147, 47 HCC and 100 intrahepatic cholangiocarcinoma (iCCA)) and Mongolia (N = 70, all HCC). We found only one HCC patient with a potentially oncogenic integration of AAV, in contrast to higher frequency reported in European patients. There were no oncogenic AAV integrations in iCCA patients. AAV genomic segments are present preferentially in the non-tumor samples of Thai patients. By analyzing the AAV genome positions of oncogenic and non-oncogenic integrated fragments, we found that almost all the putative oncogenic integrations overlap the X gene, which is present and functional only in the strain AAV2 among all fully sequenced strains. This gene content difference could explain why putative oncogenic integrations from other AAV strains have not been reported. We resolved the discrepancies in previous analyses of AAV presence in TCGA HCC samples and extended it to CCA. There are 12 TCGA samples with an AAV segment and none are in Asian patients. AAV segments are present in preferentially in TCGA non-tumor samples, like what we observed in the Thai patients.
Conclusions: Our findings suggest a minimal AAV risk of hepatocarcinogenesis in Asian liver cancer patients. The partial genome presence and positional bias of AAV integrations into the human genome has complicated analysis of possible roles of AAV in liver cancer.
Keywords: Adeno-associated virus; Gene therapy; Hepatocellular carcinoma; Intrahepatic cholangiocarcinoma; Liver cancer; Sequence analysis; Viral capture sequencing; Viral oncogenesis; Virus integration.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
