

Cost-Effectiveness of Lipid-Lowering Treatments in Young Adults
- PMID: 34763772
- PMCID: PMC8597932
- DOI: 10.1016/j.jacc.2021.08.065
Cost-Effectiveness of Lipid-Lowering Treatments in Young Adults
Erratum in
-
Corrections.J Am Coll Cardiol. 2021 Dec 21;78(25):2612. doi: 10.1016/j.jacc.2021.11.004. J Am Coll Cardiol. 2021. PMID: 34915988 No abstract available.
Abstract
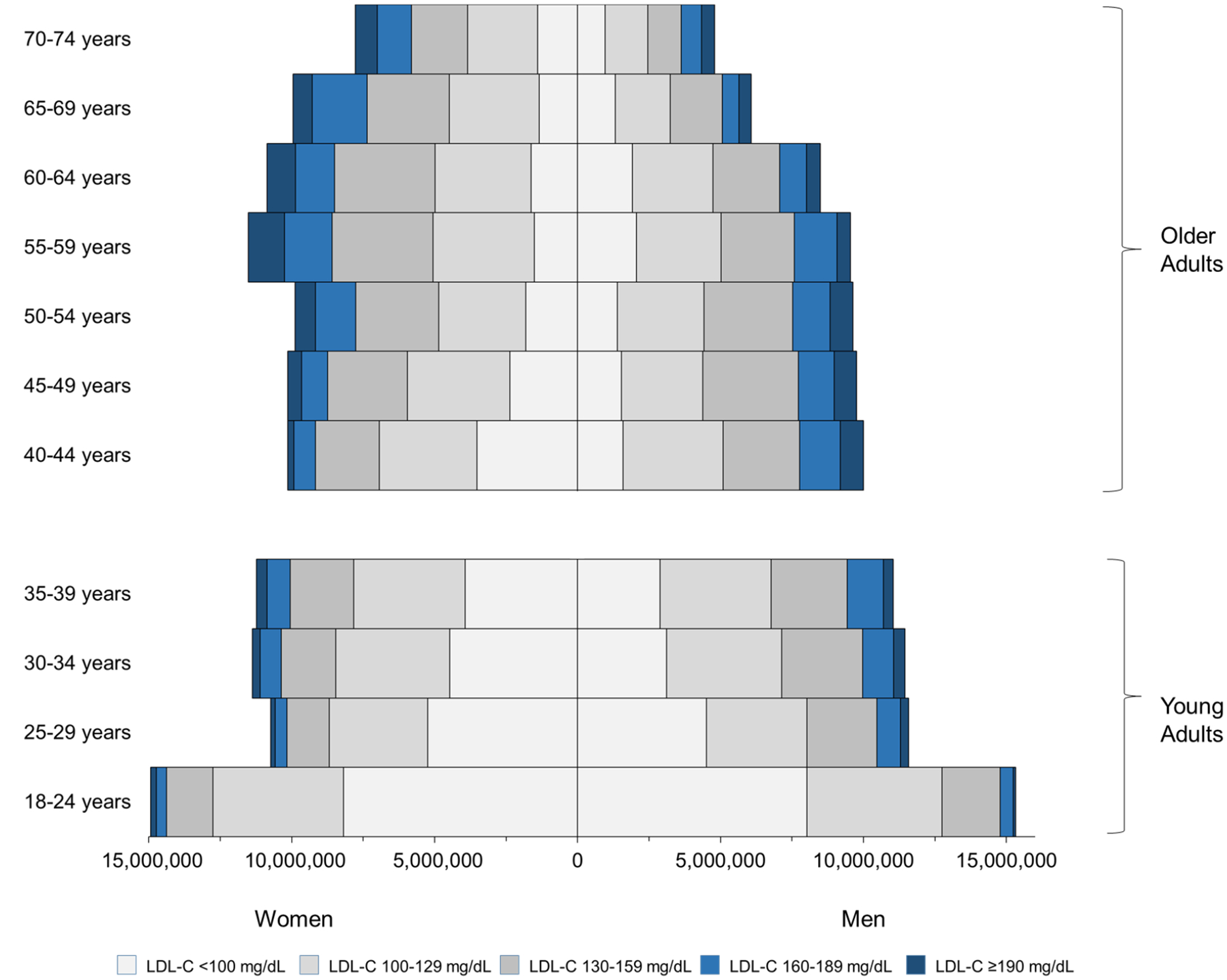
Background: Raised low-density lipoprotein cholesterol (LDL-C) in young adulthood (aged 18-39 years) is associated with atherosclerotic cardiovascular disease (ASCVD) later in life. Most young adults with elevated LDL-C do not currently receive lipid-lowering treatment.
Objectives: This study aimed to estimate the prevalence of elevated LDL-C in ASCVD-free U.S. young adults and the cost-effectiveness of lipid-lowering strategies for raised LDL-C in young adulthood compared with standard care.
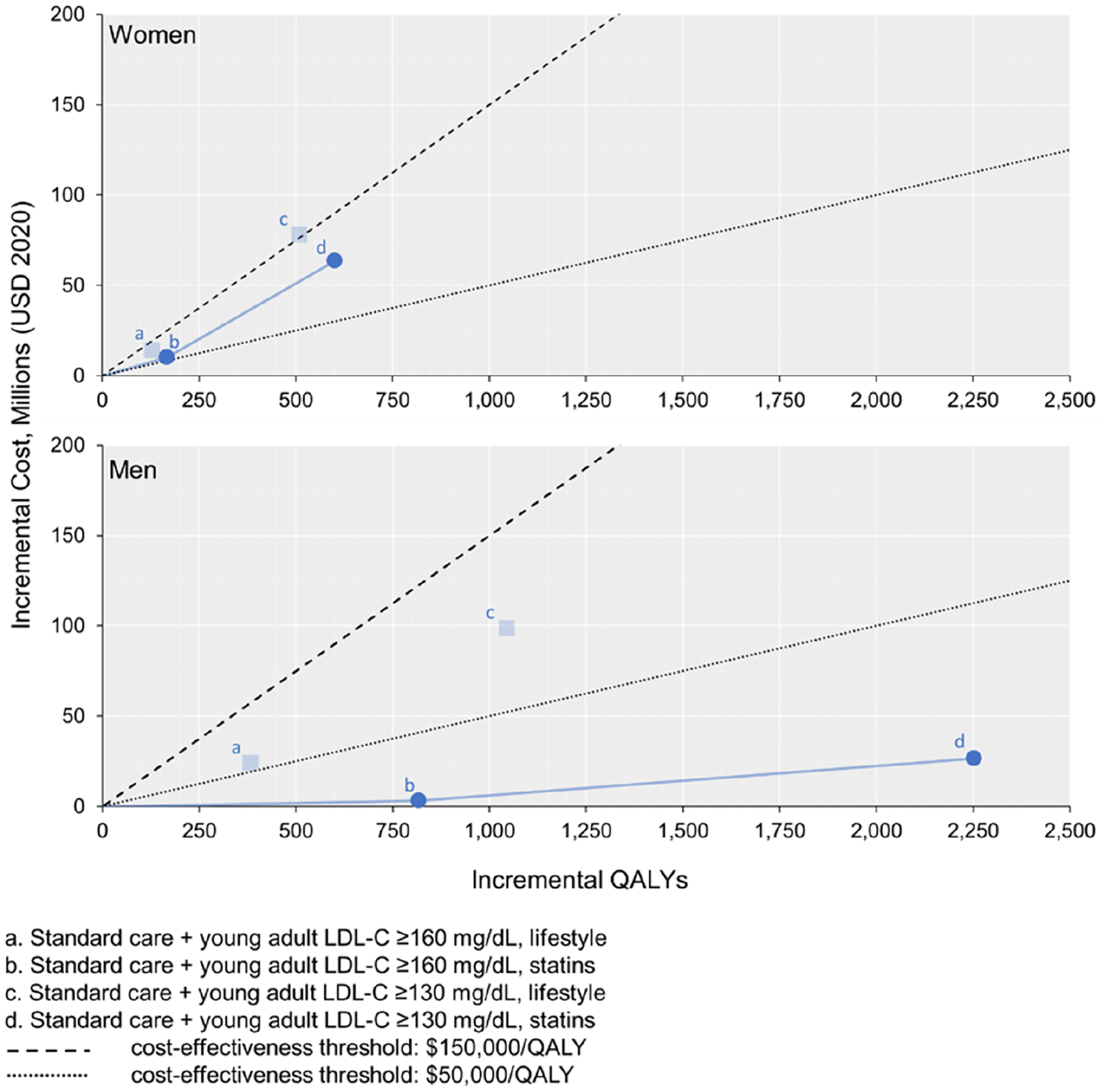
Methods: The prevalence of raised LDL-C was examined in the U.S. National Health and Nutrition Examination Survey. The CVD Policy Model projected lifetime quality-adjusted life years (QALYs), health care costs, and incremental cost-effectiveness ratios (ICERs) for lipid-lowering strategies. Standard care was statin treatment for adults aged ≥40 years based on LDL-C, ASCVD risk, or diabetes plus young adults with LDL-C ≥190 mg/dL. Lipid lowering incremental to standard care with moderate-intensity statins or intensive lifestyle interventions was simulated starting when young adult LDL-C was either ≥160 mg/dL or ≥130 mg/dL.
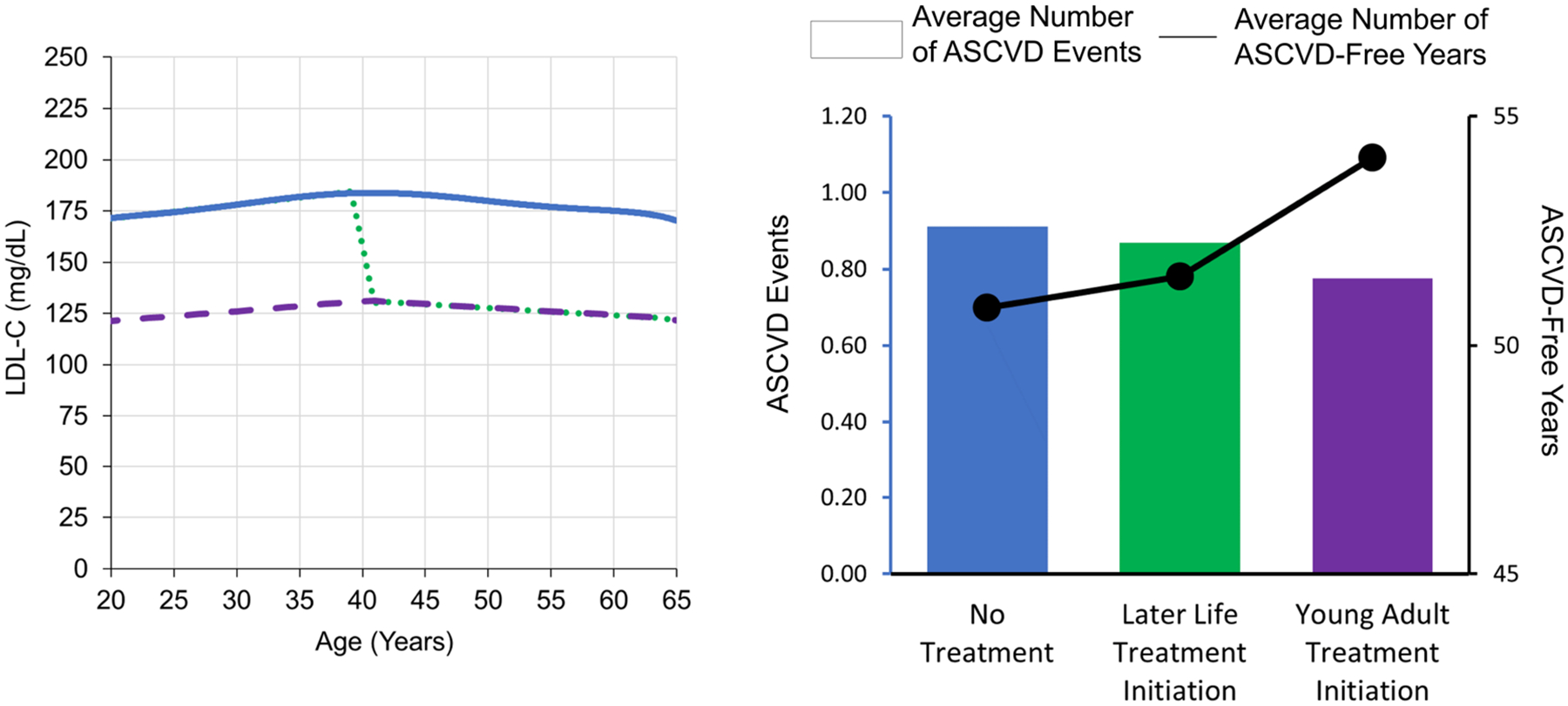
Results: Approximately 27% of ASCVD-free young adults have LDL-C of ≥130 mg/dL, and 9% have LDL-C of ≥160 mg/dL. The model projected that young adult lipid lowering with statins or lifestyle interventions would prevent lifetime ASCVD events and increase QALYs compared with standard care. ICERs were US$31,000/QALY for statins in young adult men with LDL-C of ≥130 mg/dL and US$106,000/QALY for statins in young adult women with LDL-C of ≥130 mg/dL. Intensive lifestyle intervention was more costly and less effective than statin therapy.
Conclusions: Statin treatment for LDL-C of ≥130 mg/dL is highly cost-effective in young adult men and intermediately cost-effective in young adult women.
Keywords: cardiovascular disease; cholesterol; cost-effectiveness; statins; young adulthood.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by grants R01-HL107475 and R01-HL141823 from the U.S. National Heart, Lung, and Blood Institute (NHLBI) (Dr Moran); grant DTP-1522025 from the Medical Research Council, Swindon, United Kingdom (Dr Kohli-Lynch); and NHLBI grant K01-HL140170 (Dr Bellows). The sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. Dr Kazi has received economic support from the Institute for Clinical and Economic Review outside the submitted work. Dr Moran has received grants from the NHLBI during the conduct of the study. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Time to Relax the 40-Year Age Threshold for Pharmacologic Cholesterol Lowering.J Am Coll Cardiol. 2021 Nov 16;78(20):1965-1967. doi: 10.1016/j.jacc.2021.08.072. J Am Coll Cardiol. 2021. PMID: 34763773 No abstract available.
References
-
- Mihaylova B, Emberson J, Blackwell L, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet 2012;380(9841):581–90 p 588. Doi: 10.1016/S0140-6736(12)60367-5. - DOI - PMC - PubMed
