

Post-COVID-19 assessment in a specialist clinical service: a 12-month, single-centre, prospective study in 1325 individuals
- PMID: 34764200
- PMCID: PMC8587466
- DOI: 10.1136/bmjresp-2021-001041
Post-COVID-19 assessment in a specialist clinical service: a 12-month, single-centre, prospective study in 1325 individuals
Erratum in
-
Correction: Post-COVID-19 assessment in a specialist clinical service: a 12-month, single-centre, prospective study in 1325 individuals.BMJ Open Respir Res. 2022 Jan;9(1):e001041corr1. doi: 10.1136/bmjresp-2021-001041corr1. BMJ Open Respir Res. 2022. PMID: 35064008 Free PMC article. No abstract available.
Abstract
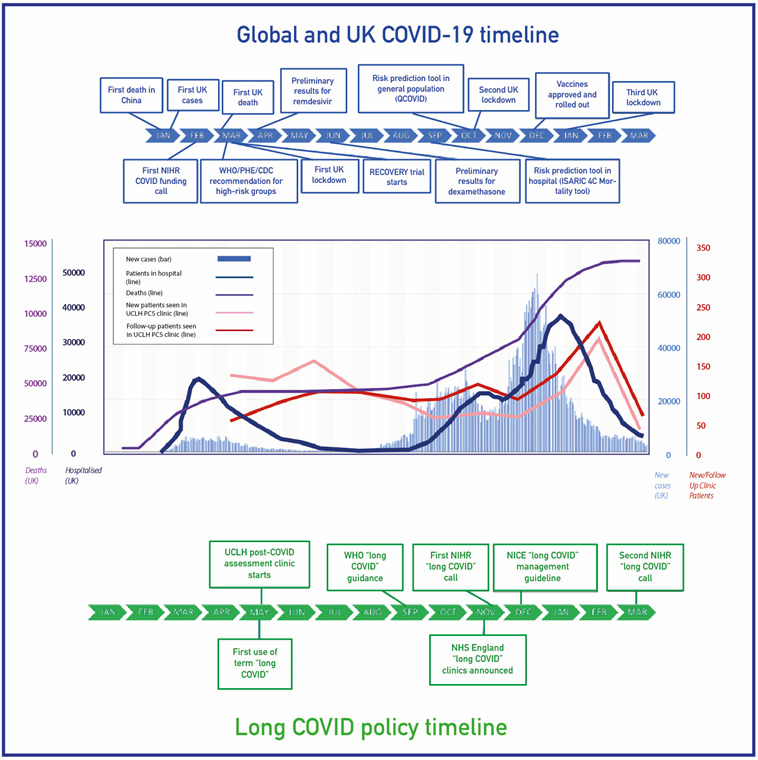
Introduction: Post-COVID-19 complications require simultaneous characterisation and management to plan policy and health system responses. We describe the 12-month experience of the first UK dedicated post-COVID-19 clinical service to include hospitalised and non-hospitalised patients.
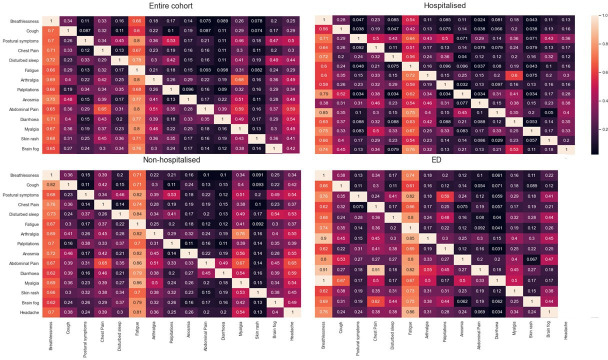
Methods: In a single-centre, observational analysis, we report the demographics, symptoms, comorbidities, investigations, treatments, functional recovery, specialist referral and rehabilitation of 1325 individuals assessed at the University College London Hospitals post-COVID-19 service between April 2020 and April 2021, comparing by referral route: posthospitalised (PH), non-hospitalised (NH) and post emergency department (PED). Symptoms associated with poor recovery or inability to return to work full time were assessed using multivariable logistic regression.
Results: 1325 individuals were assessed (PH: 547, 41.3%; PED: 212, 16%; NH: 566, 42.7%). Compared with the PH and PED groups, the NH group were younger (median 44.6 (35.6-52.8) years vs 58.3 (47.0-67.7) years and 48.5 (39.4-55.7) years), more likely to be female (68.2%, 43.0% and 59.9%), less likely to be of ethnic minority (30.9%, 52.7% and 41.0%) or seen later after symptom onset (median (IQR): 194 (118-298) days, 69 (51-111) days and 76 (55-128) days; all p<0.0001). All groups had similar rates of onward specialist referral (NH 18.7%, PH 16.1% and PED 18.9%, p=0.452) and were more likely to require support for breathlessness (23.7%, 5.5% and 15.1%, p<0.001) and fatigue (17.8%, 4.8% and 8.0%, p<0.001). Hospitalised patients had higher rates of pulmonary emboli, persistent lung interstitial abnormalities and other organ impairment. 716 (54.0%) individuals reported <75% optimal health (median 70%, IQR 55%-85%). Less than half of employed individuals could return to work full time at first assessment.
Conclusion: Post-COVID-19 symptoms were significant in PH and NH patients, with significant ongoing healthcare needs and utilisation. Trials of interventions and patient-centred pathways for diagnostic and treatment approaches are urgently required.
Keywords: COVID-19; clinical epidemiology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AB has received research grants from AstraZeneca, unrelated to this work. All other authors report no relevant conflicts of interest.
Figures

References
-
- National Institute for Health and Care Excellence . COVID-19 rapid guideline: managing the long-term effects of COVID-19, 2020. Available: https://www.nice.org.uk/guidance/ng188 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous