

Cerebral dysfunctions caused by sepsis during ageing
- PMID: 34764472
- PMCID: PMC8582341
- DOI: 10.1038/s41577-021-00643-7
Cerebral dysfunctions caused by sepsis during ageing
Abstract
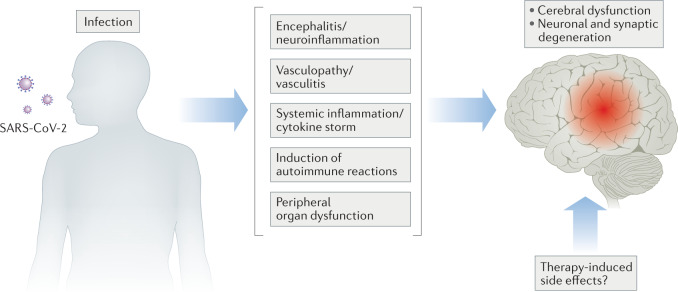
Systemic inflammation elicited by sepsis can induce an acute cerebral dysfunction known as sepsis-associated encephalopathy (SAE). Recent evidence suggests that SAE is common but shows a dynamic trajectory over time. Half of all patients with sepsis develop SAE in the intensive care unit, and some survivors present with sustained cognitive impairments for several years after initial sepsis onset. It is not clear why some, but not all, patients develop SAE and also the factors that determine the persistence of SAE. Here, we first summarize the chronic pathology and the dynamic changes in cognitive functions seen after the onset of sepsis. We then outline the cerebral effects of sepsis, such as neuroinflammation, alterations in neuronal synapses and neurovascular changes. We discuss the key factors that might contribute to the development and persistence of SAE in older patients, including premorbid neurodegenerative pathology, side effects of sedatives, renal dysfunction and latent virus reactivation. Finally, we postulate that some of the mechanisms that underpin neuropathology in SAE may also be relevant to delirium and persisting cognitive impairments that are seen in patients with severe COVID-19.
© 2021. Springer Nature Limited.
Conflict of interest statement
M.T.H. belongs to an advisory board at IFM Therapeutics and Alector. T.M. declares no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
