

Optimizing In Situ Vaccination During Radiotherapy
- PMID: 34765538
- PMCID: PMC8577814
- DOI: 10.3389/fonc.2021.711078
Optimizing In Situ Vaccination During Radiotherapy
Abstract
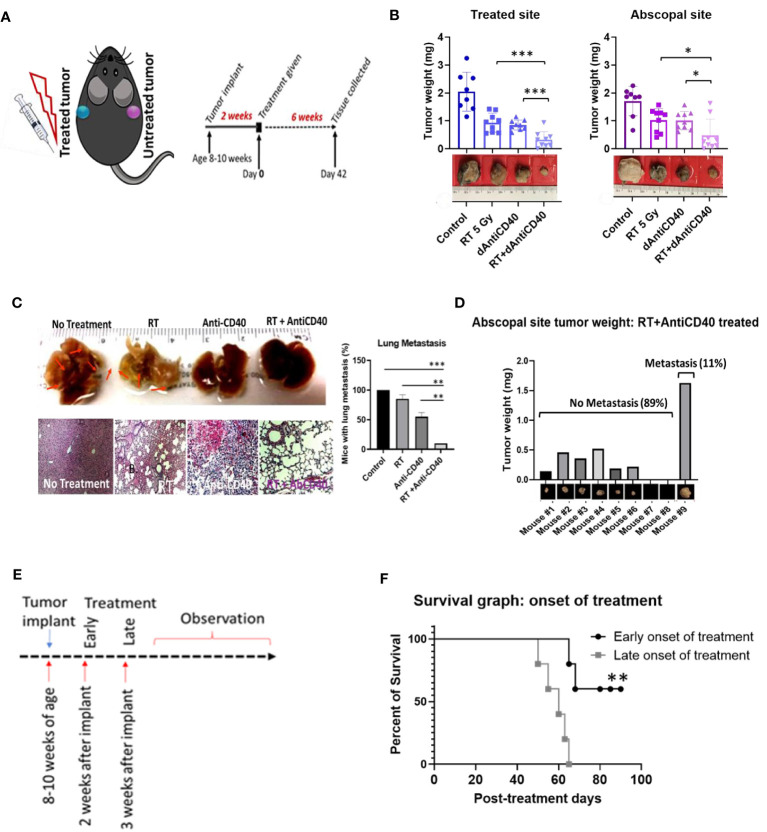
Effective in situ cancer vaccines require both a means of tumor cell death and a source of adjuvant to activate local dendritic cells. Studies have shown that the use of radiotherapy (RT) to induce tumor cell death and anti-CD40 to activate dendritic cells can result in in situ vaccination in animal models. Here, investigations are carried out on potential strategies to enhance such in situ vaccination. Strategies investigated include the use of smart immunogenic biomaterials (IBM) loaded with anti-CD40 in different tumor types including immunologically cold tumors like pancreatic and prostate tumors. The use of downstream checkpoint inhibitors to further boost such in situ vaccination is also examined. Results indicate that the use of IBM to deliver the anti-CD40 significantly enhances the effectiveness of in situ vaccination with anti-CD40 compared with direct injection in pancreatic and prostate cancers (p < 0.001 and p < 0.0001, respectively). This finding is consistent with significant increase in infiltration of antigen-presenting cells in the treated tumor, and significant increase in the infiltration of CD8+ cytotoxic T lymphocyte into distant untreated tumors. Moreover, in situ vaccination with IBM is consistently observed across different tumor types. Meanwhile, the addition of downstream immune checkpoint inhibitors further enhances overall survival when using the IBM approach. Overall, the findings highlight potential avenues for enhancing in situ vaccination when combining radiotherapy with anti-CD40.
Keywords: abscopal effect; cancer vaccine; dose-painting; immunogenic biomaterials; immunotherapy; pancreatic cancer; prostate cancer; radiotherapy.
Copyright © 2021 Yasmin-Karim, Wood, Wirtz, Moreau, Bih, Swanson, Muflam, Ainsworth, Ziberi and Ngwa.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Golden EB, Chhabra A, Chachoua A, Adams S, Donach M, Fenton-Kerimian M, et al. Local Radiotherapy and Granulocyte-Macrophage Colony-Stimulating Factor to Generate Abscopal Responses in Patients With Metastatic Solid Tumours: A Proof-of-Principle Trial. Lancet Oncol (2015) 16:795–803. doi: 10.1016/S1470-2045(15)00054-6 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials