

A Rare Case of Subcutaneous Insulin Resistance Presumed to be due to Paraneoplastic Process in Pancreatic Adenocarcinoma
- PMID: 34765736
- PMCID: PMC8573285
- DOI: 10.1016/j.aace.2021.06.001
A Rare Case of Subcutaneous Insulin Resistance Presumed to be due to Paraneoplastic Process in Pancreatic Adenocarcinoma
Abstract
Objective: We describe a rare case of profound subcutaneous insulin resistance (SIR) presumed due to a paraneoplastic process caused by pancreatic adenocarcinoma that improved with intravenous insulin and tumor resection.
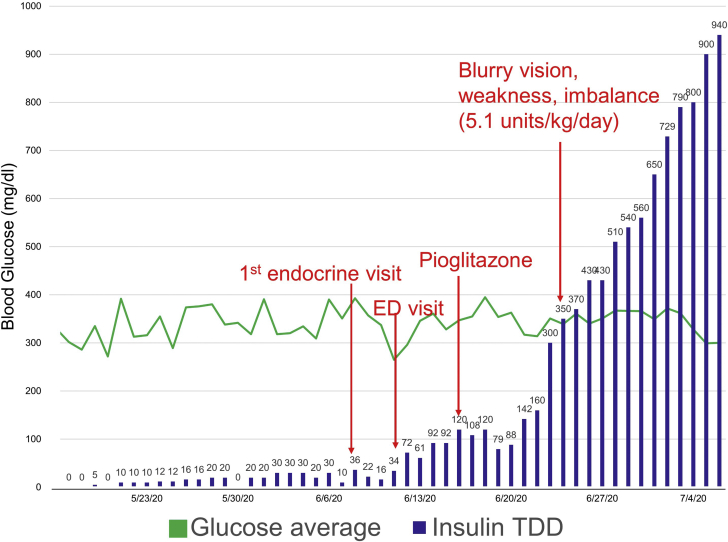
Methods: An 80-year-old man with previously well-controlled type 2 diabetes mellitus had worsening glycemic control (hemoglobin A1C increase of 6.5% to 8.6% over 4 months) following a recent diagnosis of pancreatic adenocarcinoma. His blood glucose was uncontrolled at 600 mg/dL despite rapid up-titration of a subcutaneous basal-bolus insulin regimen totaling 1000 units/d. Extensive evaluation of insulin resistance including insulin antibodies and anti-insulin receptor antibodies was negative. Due to clinical deterioration, the patient underwent pancreaticoduodenectomy before the completion of neoadjuvant chemotherapy. The patient received intravenous insulin before surgery, which resulted in rapid improvement in glycemic control. The patient's blood glucose normalized, and he was maintained on metformin monotherapy following pancreaticoduodenectomy.
Results: This patient had evidence of SIR in the setting of pancreatic adenocarcinoma. SIR was likely a paraneoplastic process as glycemic control improved after tumor resection. Interestingly, the patient did not have hyperinsulinemia but rather evidence of β-cell dysfunction, which highlights the possibility of exogenous insulin resistance.
Conclusion: Paraneoplastic processes due to pancreatic adenocarcinoma can cause SIR, marked by profound hyperglycemia and deteriorating functional status. It is, therefore important to recognize this rare syndrome and appropriately escalate to a higher level of care and consider proceeding with tumor resection.
Keywords: AG, average blood glucose; CGM, continuous glucose monitor; HOMA-IR, homeostatic model assessment of insulin resistance; IV, intravenous; SD, standard deviation; SIR, subcutaneous insulin resistance; T2DM, type 2 diabetes mellitus; pancreatic adenocarcinoma; paraneoplastic syndrome; subcutaneous insulin resistance.
© 2021 AACE. Published by Elsevier Inc.
Figures

References
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. - PubMed
-
- Everhart J., Wright D. Diabetes mellitus as a risk factor for pancreatic cancer. A meta-analysis. JAMA. 1995;273(20):1605–1609. - PubMed
-
- Gullo L., Pezzilli R., Morselli-Labate A.M., Italian Pancreatic Cancer Study Group Diabetes and the risk of pancreatic cancer. N Engl J Med. 1994;331(2):81–84. - PubMed
-
- Permert J., Ihse I., Jorfeldt L., von Schenck H., Arnquist H.J., Larsson J. Improved glucose metabolism after subtotal pancreatectomy for pancreatic cancer. Br J Surg. 1993;80(8):1047–1050. - PubMed
-
- Hines G., Kennedy I., Stevens R., Matthews D., Levy J. A calculator for HOMA. 2004;suppl 1:A222.
Publication types
LinkOut - more resources
Full Text Sources