

Net effects of sodium-glucose co-transporter-2 inhibition in different patient groups: a meta-analysis of large placebo-controlled randomized trials
- PMID: 34765951
- PMCID: PMC8571171
- DOI: 10.1016/j.eclinm.2021.101163
Net effects of sodium-glucose co-transporter-2 inhibition in different patient groups: a meta-analysis of large placebo-controlled randomized trials
Abstract
Background: The net absolute effects of sodium-glucose co-transporter-2 (SGLT-2) inhibitors across different patient groups have not been quantified.
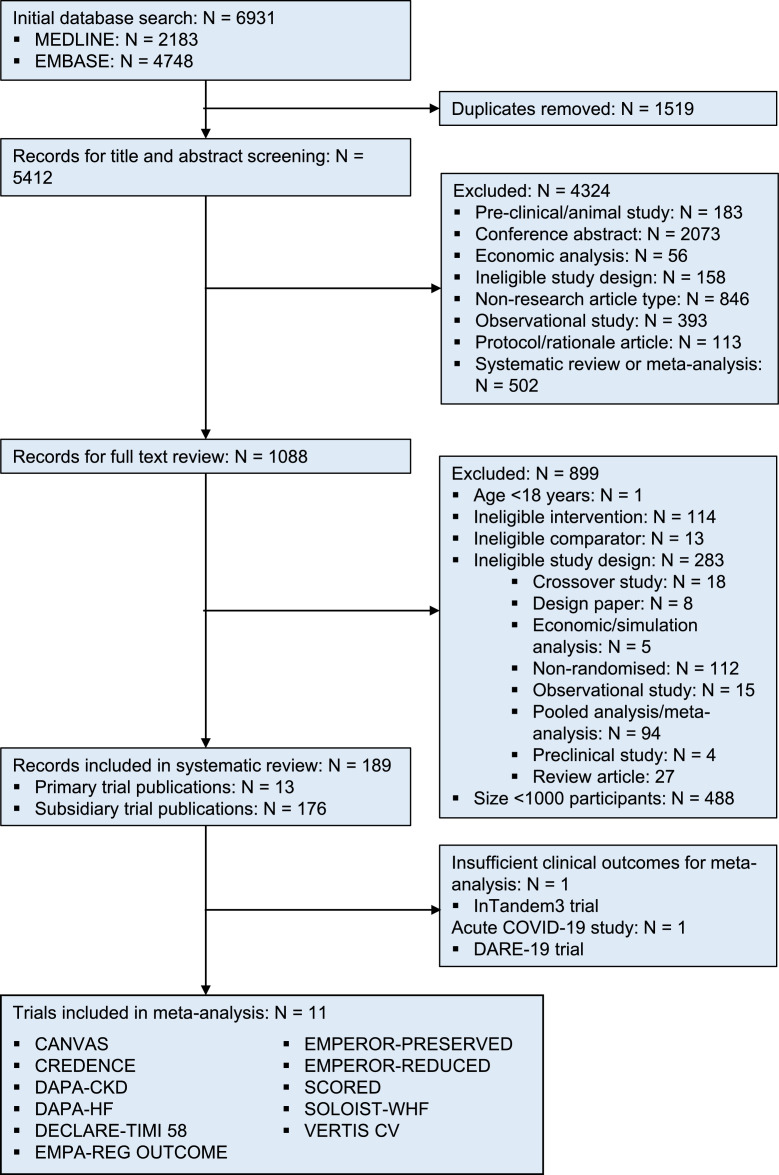
Methods: We performed a meta-analysis of published large (>500 participants/arm) placebo-controlled SGLT-2 inhibitor trials after systematically searching MEDLINE and Embase databases from inception to 28th August 2021 (PROSPERO 2021 CRD42021240468).
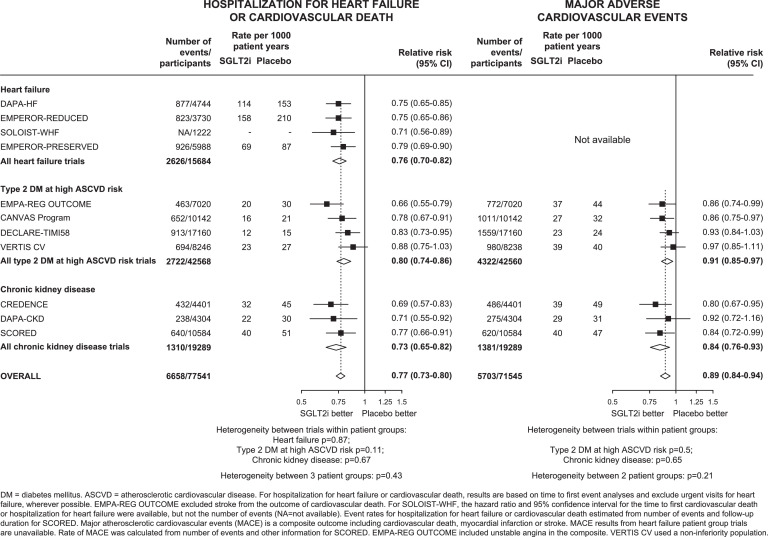
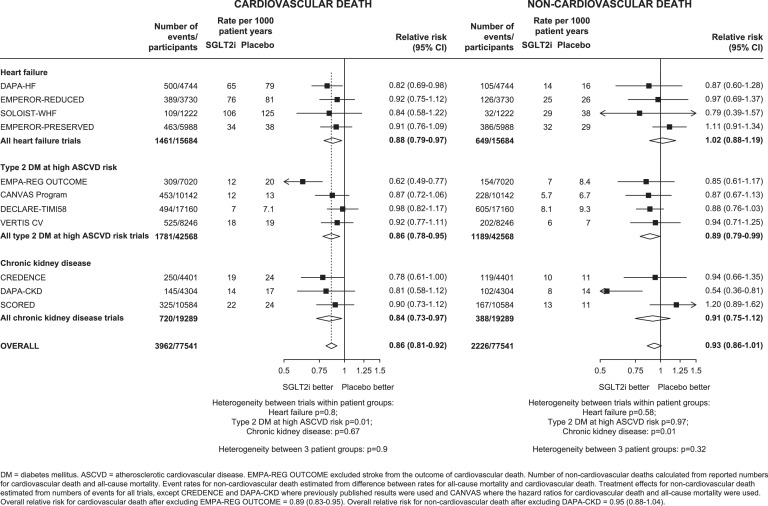
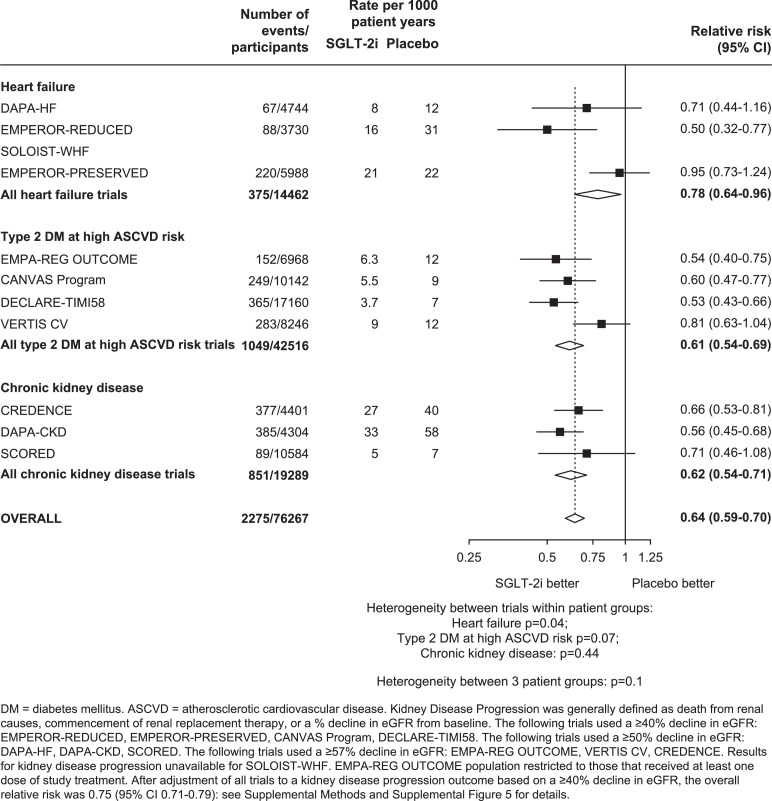
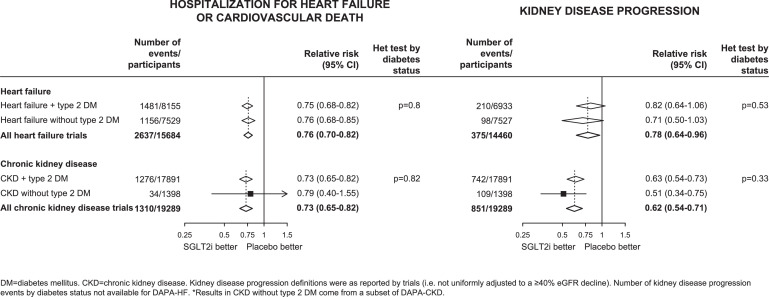
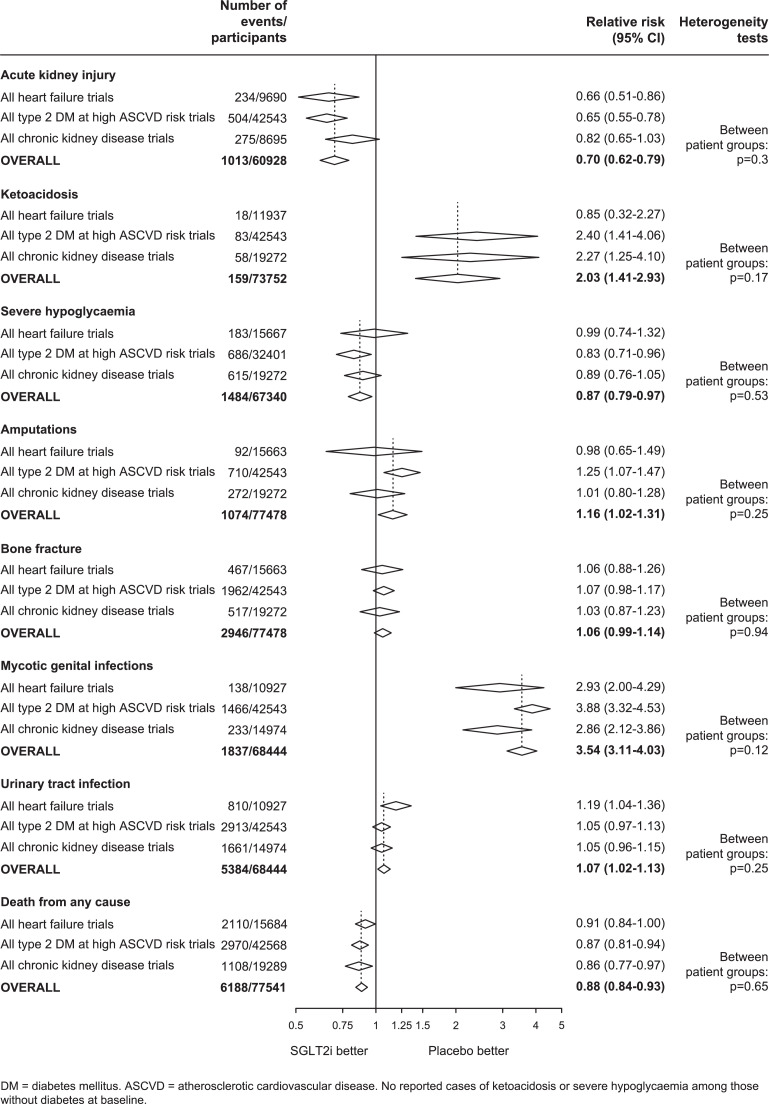
Findings: Four heart failure trials (n=15,684 participants), four trials in type 2 diabetes mellitus at high atherosclerotic cardiovascular risk (n=42,568), and three trials in chronic kidney disease (n=19,289) were included. Relative risks (RRs) for all cardiovascular, renal and safety outcomes were broadly similar across these three patient groups, and between people with or without diabetes. Overall, compared to placebo, allocation to SGLT-2 inhibition reduced risk of hospitalization for heart failure or cardiovascular death by 23% (RR=0.77, 95%CI 0.73-0.80; n=6658), cardiovascular death by 14% (0.86, 0.81-0.92; n=3962), major adverse cardiovascular events by 11% (0.89, 0.84-0.94; n=5703), kidney disease progression by 36% (0.64, 0.59-0.70; n=2275), acute kidney injury by 30% (0.70, 0.62-0.79; n=1013 events) and severe hypoglycaemia by 13% (0.87, 0.79-0.97; n=1484). There was no effect of SGLT-2 inhibition on risk of non-cardiovascular death (0.93, 0.86-1.01; n=2226), but a net 12% reduction in all-cause mortality remained evident (0.88, 0.84-0.93; n=6188). However, the risk of ketoacidosis was 2-times higher among those allocated SGLT-2 inhibitors compared to placebo (2.03, 1.41-2.93; n=159; absolute excess in people with diabetes ∼0.3/1000 patient years). A small increased risk of urinary tract infection was evident (1.07, 1.02-1.13; n=5384) alongside a known increased risk of mycotic genital infections. Overall, risk of lower limb amputations was increased by 16% (1.16, 1.02-1.31; n=1074), but this risk was largely driven by a single outlying trial (CANVAS).
Interpretations: The relative effects of SGLT-2 inhibition on key safety and efficacy outcomes are consistent across the different studied groups of patient. Consequently, absolute benefits and harms are determined by the absolute baseline risk of particular outcomes, with absolute benefits on mortality and on non-fatal serious cardiac/renal outcomes substantially exceeding the risks of amputation and ketoacidosis in the main patient groups studied to date.
Funding: MRC-UK & KRUK.
Keywords: CKD; Heart failure; Randomized trials; Safety; Sodium-glucose co-transporter 2 inhibitors.
© 2021 The Author(s).
Conflict of interest statement
CTSU has a staff policy of not accepting honoraria or other payments from the pharmaceutical industry, expect for the reimbursement of costs to participate in scientific meetings. NS, JE, CR, CB, RH, and WGH report a grant paid to their institution by Boehringer Ingelheim. SB reports honoraria from Astra Zeneca and Napp. CR is on the Board of Directors for CDISC and reports funding from the British Heart Foundation. RH and WGH also report grants paid to their institution from Novartis, Roche, and Regeneron. CB, CR, and WGH report funding from MRC-UK. WGH reports personal funding from Kidney Research UK and is co-chair of the UK Kidney Association's clinical guideline for use of SGLT-2 inhibitors in adults with chronic kidney disease. All the other authors report no conflicts.
Figures
References
-
- Food and Drug Administration . 2021. Guidance for Industry on Diabetes Mellitus-Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes. A Notice by the Food and Drug Administration on 12/19/2008.https://www.federalregister.gov/documents/2008/12/19/E8-30086/guidance-f... (accessed 1st January)
-
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015;373(22):2117–2128. - PubMed
-
- Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med. 2017;377(7):644–657. - PubMed
-
- Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2019;380(4):347–357. - PubMed
-
- Cannon CP, Pratley R, Dagogo-Jack S, Mancuso J, Huyck S, Masiukiewicz U. Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes. N Engl J Med. 2020;383(15):1425–1435. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
