

Atypical lymphocytes in the peripheral blood of COVID-19 patients: A prognostic factor for the clinical course of COVID-19
- PMID: 34767614
- PMCID: PMC8589156
- DOI: 10.1371/journal.pone.0259910
Atypical lymphocytes in the peripheral blood of COVID-19 patients: A prognostic factor for the clinical course of COVID-19
Abstract
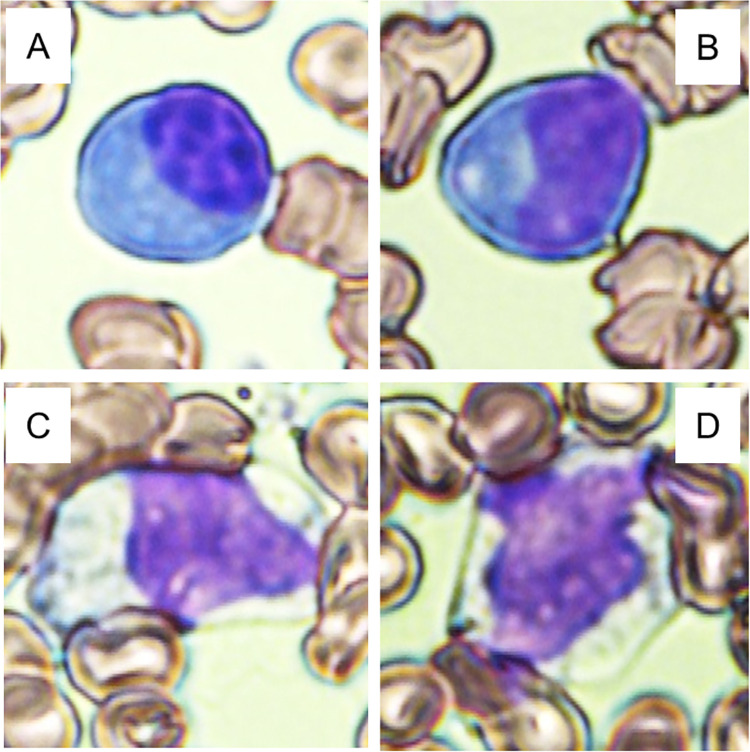
Background: Clinical observations have shown that there is a relationship between coronavirus disease 2019 (COVID-19) and atypical lymphocytes in the peripheral blood; however, knowledge about the time course of the changes in atypical lymphocytes and the association with the clinical course of COVID-19 is limited.
Objective: Our purposes were to investigate the dynamics of atypical lymphocytes in COVID-19 patients and to estimate their clinical significance for diagnosis and monitoring disease course.
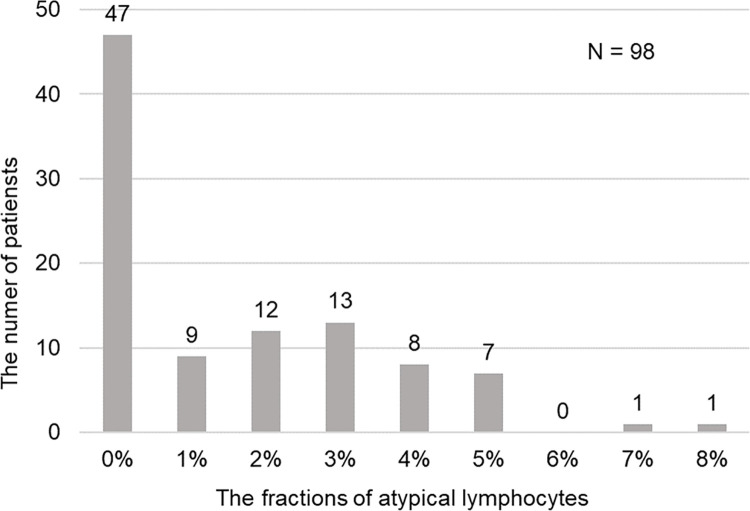
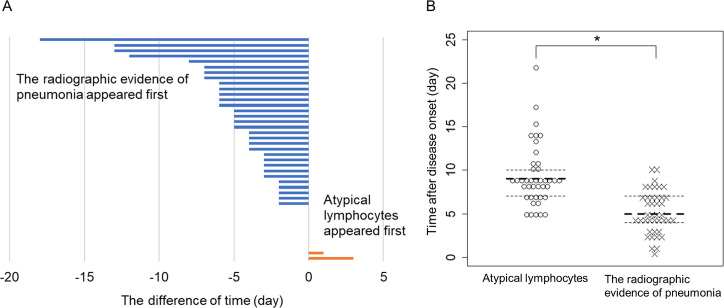
Materials and methods: We retrospectively identified 98 inpatients in a general ward at Kashiwa Municipal Hospital from May 1st, 2020, to October 31st, 2020. We extracted data on patient demographics, symptoms, comorbidities, blood test results, radiographic findings, treatment after admission and clinical course. We compared clinical findings between patients with and without atypical lymphocytes, investigated the behavior of atypical lymphocytes throughout the clinical course of COVID-19, and determined the relationships among the development of pneumonia, the use of supplemental oxygen and the presence of atypical lymphocytes.
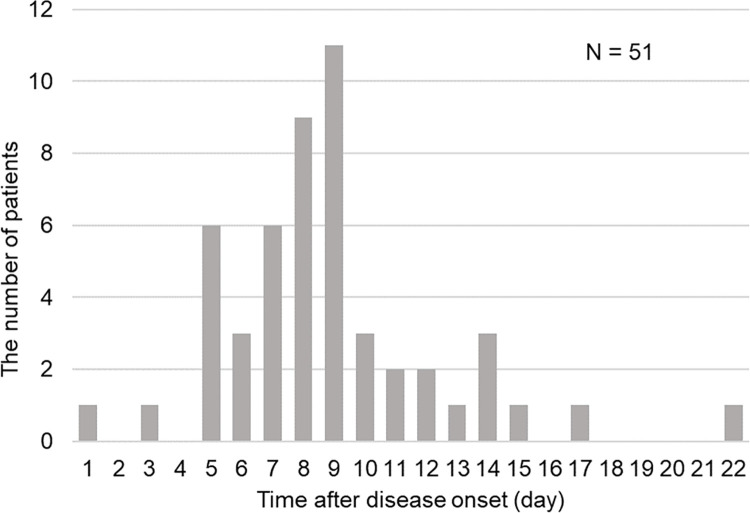
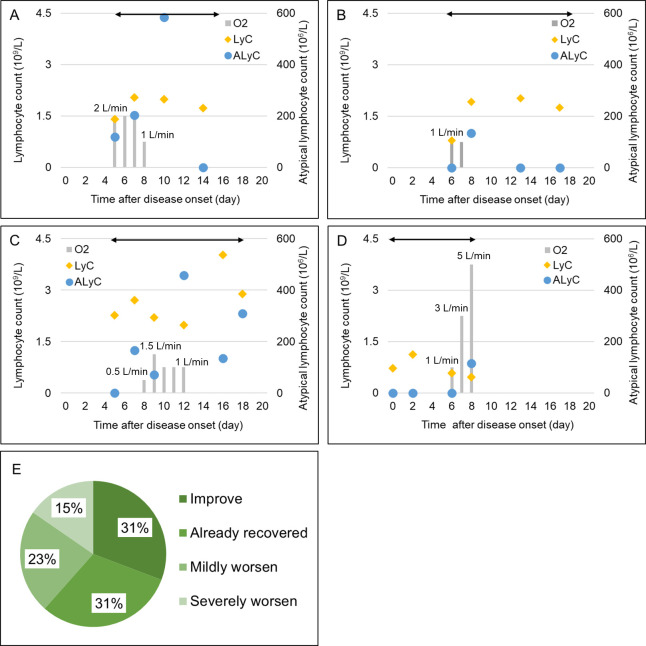
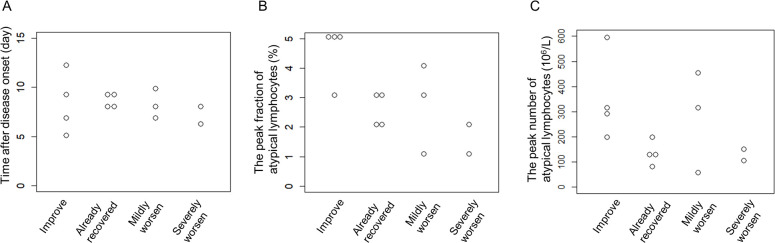
Results: Patients with atypical lymphocytes had a significantly higher prevalence of pneumonia (80.4% vs. 42.6%, p < 0.0001) and the use of supplemental oxygen (25.5% vs. 4.3%, p = 0.0042). The median time to the appearance of atypical lymphocytes after disease onset was eight days, and atypical lymphocytes were observed in 16/98 (16.3%) patients at the first visit. Atypical lymphocytes appeared after the confirmation of lung infiltrates in 31/41 (75.6%) patients. Of the 13 oxygen-treated patients with atypical lymphocytes, approximately two-thirds had a stable or improved clinical course after the appearance of atypical lymphocytes.
Conclusion: Atypical lymphocytes frequently appeared in the peripheral blood of COVID-19 patients one week after disease onset. Patients with atypical lymphocytes were more likely to have pneumonia and to need supplemental oxygen; however, two-thirds of them showed clinical improvement after the appearance of atypical lymphocytes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Prolonged prothrombin time as an early prognostic indicator of severe acute respiratory distress syndrome in patients with COVID-19 related pneumonia.Curr Med Res Opin. 2021 Jan;37(1):21-25. doi: 10.1080/03007995.2020.1853510. Epub 2020 Dec 7. Curr Med Res Opin. 2021. PMID: 33210948 Free PMC article.
-
Bacterial and fungal coinfection among hospitalized patients with COVID-19: a retrospective cohort study in a UK secondary-care setting.Clin Microbiol Infect. 2020 Oct;26(10):1395-1399. doi: 10.1016/j.cmi.2020.06.025. Epub 2020 Jun 27. Clin Microbiol Infect. 2020. PMID: 32603803 Free PMC article.
-
SARS-CoV-2 and COVID-19 for the ophthalmologist.Clin Exp Ophthalmol. 2021 Jan;49(1):70-80. doi: 10.1111/ceo.13877. Epub 2020 Nov 9. Clin Exp Ophthalmol. 2021. PMID: 33131139 Review.
-
The impact of the SARS-CoV-2 pandemic on the prevalence of respiratory tract pathogens in patients with community-acquired pneumonia in Germany.Emerg Microbes Infect. 2021 Dec;10(1):1515-1518. doi: 10.1080/22221751.2021.1957402. Emerg Microbes Infect. 2021. PMID: 34269641 Free PMC article.
-
Pathogenesis-directed therapy of 2019 novel coronavirus disease.J Med Virol. 2021 Mar;93(3):1320-1342. doi: 10.1002/jmv.26610. Epub 2020 Nov 10. J Med Virol. 2021. PMID: 33073355 Review.
Cited by
-
The Impact of Past COVID-19 Infection on Selected Lymphocyte Subsets in Pediatric Patients.Vaccines (Basel). 2023 Mar 15;11(3):659. doi: 10.3390/vaccines11030659. Vaccines (Basel). 2023. PMID: 36992243 Free PMC article.
-
Characteristics and clinical outcomes of COVID-19 in children: a hospital-based surveillance study in Latin America's hardest-hit city.IJID Reg. 2023 Jun;7:52-62. doi: 10.1016/j.ijregi.2022.12.003. Epub 2022 Dec 15. IJID Reg. 2023. PMID: 36536932 Free PMC article.
-
Morphological abnormalities of peripheral blood cells among patients with COVID-19 disease.Heliyon. 2024 Jan 17;10(2):e24527. doi: 10.1016/j.heliyon.2024.e24527. eCollection 2024 Jan 30. Heliyon. 2024. PMID: 38304781 Free PMC article.
-
Are atypical lymphocytes a new predictive factor in the development of COVID-19?Rev Soc Bras Med Trop. 2022 Sep 19;55:e0154. doi: 10.1590/0037-8682-0154-2022. eCollection 2022. Rev Soc Bras Med Trop. 2022. PMID: 36134860 Free PMC article. No abstract available.
References
-
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard: World Health Organization; 2021. [cited 2021 29 Apr]. Available from: doi: 10.1038/s41564-021-00961-5 - DOI
-
- Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, et al.., editors. Harrison’s Principles of Internal Medicine. 17th ed. New York: McGraw-Hill Professional; 2008.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
