

Innate immune defenses at the maternal-fetal interface
- PMID: 34768027
- PMCID: PMC11063961
- DOI: 10.1016/j.coi.2021.10.007
Innate immune defenses at the maternal-fetal interface
Abstract
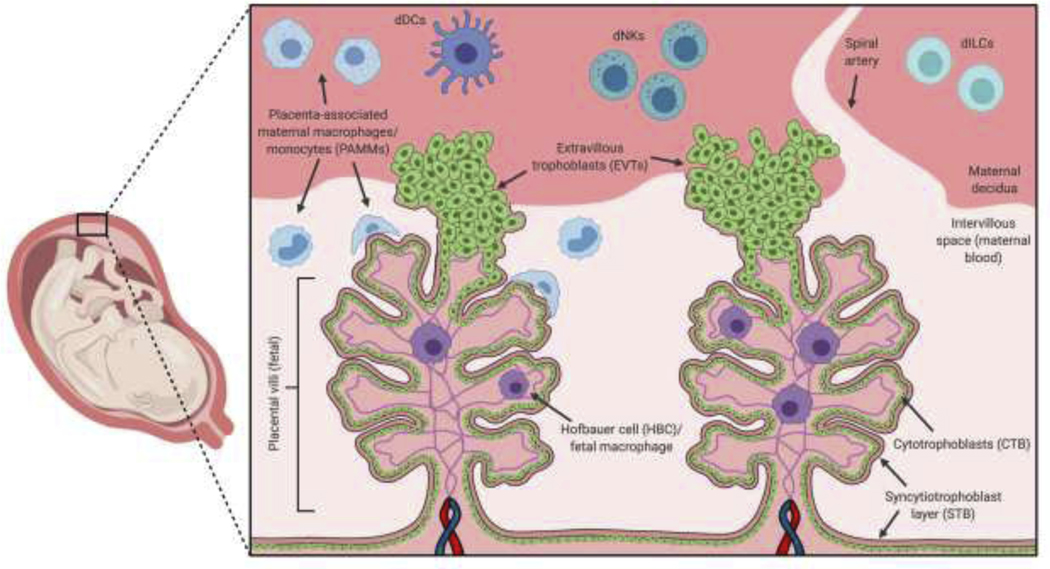
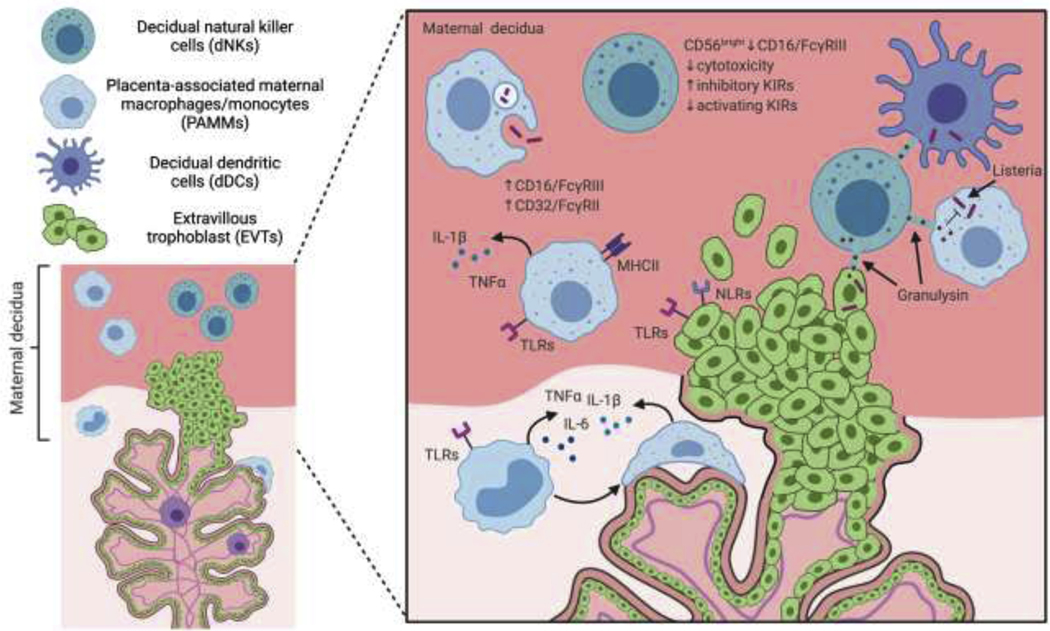
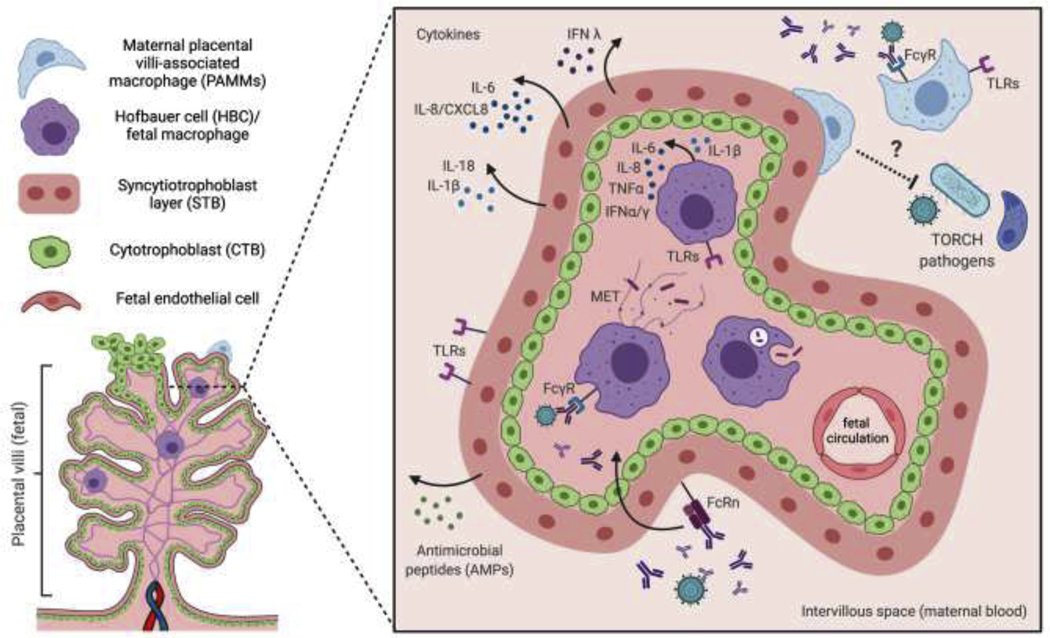
The human maternal-fetal interface is an immunologically complex environment that must balance the divergent demands of tolerance towards the developing fetus with anti-pathogen defense. The innate immune responses at the maternal-fetal interface that function in anti-microbial defense have been understudied to-date and how 'TORCH' pathogens evade maternal innate immunity to infect the fetus remains poorly understood. Herein, we discuss how newly described decidual innate lymphoid cells and maternal placenta-associated macrophage subsets may be involved in anti-pathogen defense. Moreover, we outline recent advances in our understanding of how placental trophoblasts and fetal-derived macrophages (Hofbauer cells) function in anti-microbial defense. In summary, we highlight current gaps in knowledge and describe novel experimental models of the human decidua and placenta that are poised to advance our knowledge of innate immune defenses at the maternal-fetal interface.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Innate immune signaling in trophoblast and decidua organoids defines differential antiviral defenses at the maternal-fetal interface.Elife. 2022 Aug 17;11:e79794. doi: 10.7554/eLife.79794. Elife. 2022. PMID: 35975985 Free PMC article.
-
Innate Immune Mechanisms to Protect Against Infection at the Human Decidual-Placental Interface.Front Immunol. 2020 Sep 10;11:2070. doi: 10.3389/fimmu.2020.02070. eCollection 2020. Front Immunol. 2020. PMID: 33013876 Free PMC article. Review.
-
Zika Virus Infects Early- and Midgestation Human Maternal Decidual Tissues, Inducing Distinct Innate Tissue Responses in the Maternal-Fetal Interface.J Virol. 2017 Jan 31;91(4):e01905-16. doi: 10.1128/JVI.01905-16. Print 2017 Feb 15. J Virol. 2017. PMID: 27974560 Free PMC article.
-
Interleukin-34 is present at the fetal-maternal interface and induces immunoregulatory macrophages of a decidual phenotype in vitro.Hum Reprod. 2018 Apr 1;33(4):588-599. doi: 10.1093/humrep/dey037. Hum Reprod. 2018. PMID: 29579271
-
The maternal-fetal interface at single-cell resolution: uncovering the cellular anatomy of the placenta and decidua.Am J Obstet Gynecol. 2025 Apr;232(4S):S55-S79. doi: 10.1016/j.ajog.2024.12.032. Am J Obstet Gynecol. 2025. PMID: 40253083 Review.
Cited by
-
Placental Inflammation in Preterm Premature Rupture of Membranes and Risk of Neurodevelopmental Disorders.Cells. 2025 Jun 24;14(13):965. doi: 10.3390/cells14130965. Cells. 2025. PMID: 40643486 Free PMC article. Review.
-
Trem2/Syk/PI3K axis contributes to the host protection against Toxoplasma gondii-induced adverse pregnancy outcomes via modulating decidual macrophages.PLoS Pathog. 2024 Sep 9;20(9):e1012543. doi: 10.1371/journal.ppat.1012543. eCollection 2024 Sep. PLoS Pathog. 2024. PMID: 39250507 Free PMC article.
-
Fetal inflammatory response at the fetomaternal interface: A requirement for labor at term and preterm.Immunol Rev. 2022 Jul;308(1):149-167. doi: 10.1111/imr.13075. Epub 2022 Mar 14. Immunol Rev. 2022. PMID: 35285967 Free PMC article. Review.
-
Roles of TGF-β1 in Viral Infection during Pregnancy: Research Update and Perspectives.Int J Mol Sci. 2023 Mar 30;24(7):6489. doi: 10.3390/ijms24076489. Int J Mol Sci. 2023. PMID: 37047462 Free PMC article. Review.
-
Innate immune responses to pathogens at the maternal-fetal interface.Nat Rev Immunol. 2025 Jun 18. doi: 10.1038/s41577-025-01191-0. Online ahead of print. Nat Rev Immunol. 2025. PMID: 40533582 Review.
References
-
- Turco MY, Moffett A: Development of the human placenta. Development 2019, 146. - PubMed
-
- Pereira L: Congenital Viral Infection: Traversing the Uterine-Placental Interface. Annu Rev Virol 2018, 5:273–299. - PubMed
-
-
Vento-Tormo R, Efremova M, Botting RA, Turco MY, Vento-Tormo M, Meyer KB, Park JE,Stephenson E, Polański K, Goncalves A, et al.: Single-cell reconstruction of the early maternal-fetal interface in humans. Nature. 2018. Nov;563(7731):347–353.
** outstanding interest
Leveraging single-cell RNA sequencing from first trimester maternal decidua and fetal placental tissue, Vento Tormo et al. have assembled an exceptional “single-cell atlas” of the non-immune and immune cells at the human maternal-fetal interface. Their findings highlight the previously underappreciated heterogeneity of many decidual cell subsets, define 3 major populations of decidual NK cells (dNKs), and describe the immunoregulatory mechanisms underpinning how dNKs promote a healthy pregnancy.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
