

Predicting the Exception-CRP and Primary Hip Arthroplasty
- PMID: 34768504
- PMCID: PMC8584609
- DOI: 10.3390/jcm10214985
Predicting the Exception-CRP and Primary Hip Arthroplasty
Abstract
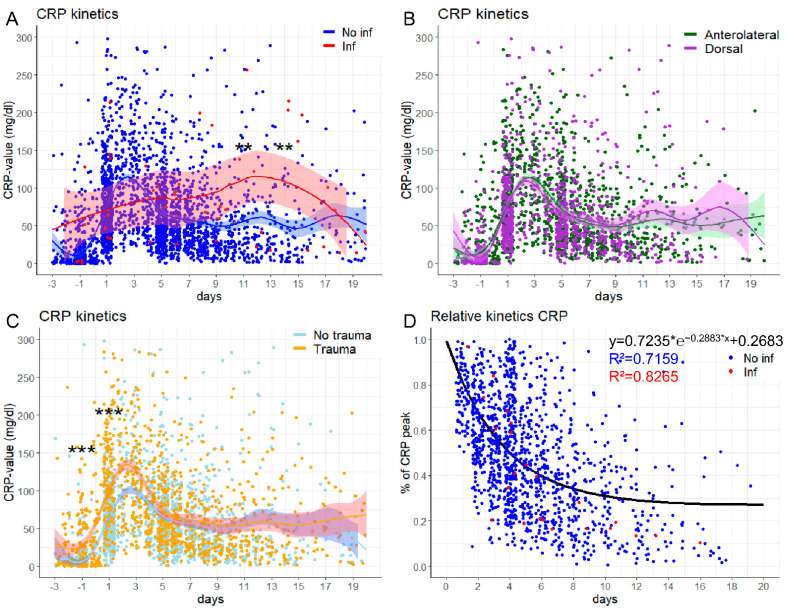
Background: While primary hip arthroplasty is the most common operative procedure in orthopedic surgery, a periprosthetic joint infection is its most severe complication. Early detection and prediction are crucial. In this study, we aimed to determine the value of postoperative C-reactive protein (CRP) and develop a formula to predict this rare, but devastating complication.
Methods: We retrospectively evaluated 708 patients with primary hip arthroplasty. CRP, white blood cell count (WBC), and several patient characteristics were assessed for 20 days following the operative procedure.
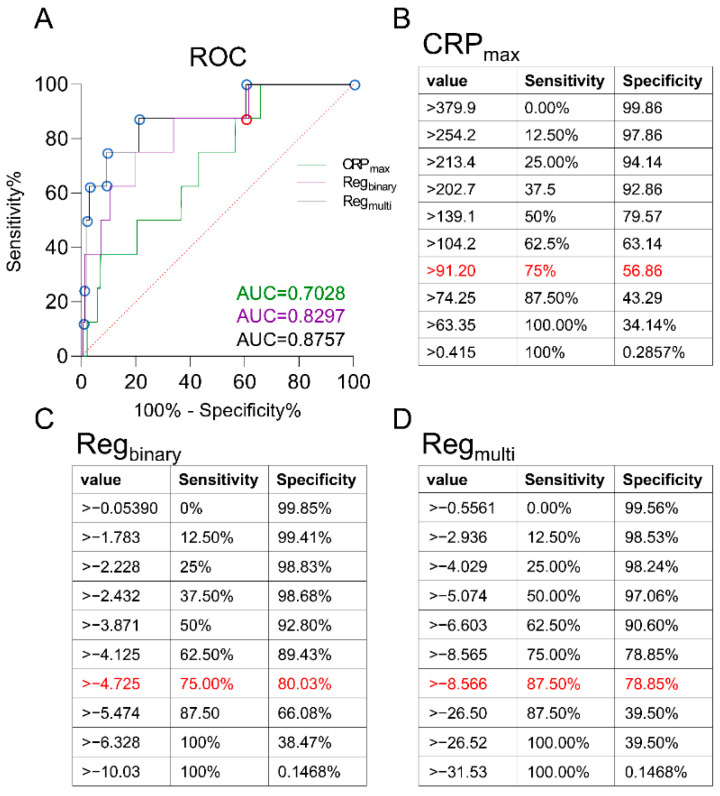
Results: Eight patients suffered an early acute periprosthetic infection. The maximum CRP predicted an infection with a sensitivity and specificity of 75% and 56.9%, respectively, while a binary logistic regression reached values of 75% and 80%. A multinominal logistic regression, however, was able to predict an early infection with a sensitivity and specificity of 87.5% and 78.9%. With a one-phase decay, 71.6% of the postoperative CRP-variance could be predicted.
Conclusion: To predict early acute periprosthetic joint infection after primary hip arthroplasty, a multinominal logistic regression is the most promising approach. Including five parameters, an early infection can be predicted on day 5 after the operative procedure with 87.5% sensitivity, while it can be excluded with 78.9% specificity.
Keywords: C-reactive protein; CRP; orthopedic surgery; periprosthetic joint infection; primary hip arthroplasty; revision surgery.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
C-reactive protein during the first 6 postoperative days after total hip arthroplasty cannot predict early periprosthetic infection.Arch Orthop Trauma Surg. 2023 Jun;143(6):3495-3503. doi: 10.1007/s00402-022-04565-4. Epub 2022 Aug 9. Arch Orthop Trauma Surg. 2023. PMID: 35943586 Free PMC article.
-
Diagnostic Value of Synovial White Blood Cell Count and Serum C-Reactive Protein for Acute Periprosthetic Joint Infection After Knee Arthroplasty.J Arthroplasty. 2017 Dec;32(12):3724-3728. doi: 10.1016/j.arth.2017.07.013. Epub 2017 Jul 18. J Arthroplasty. 2017. PMID: 28800858
-
C-reactive protein course during the first 5 days after total knee arthroplasty cannot predict early prosthetic joint infection.Arch Orthop Trauma Surg. 2017 Aug;137(8):1115-1119. doi: 10.1007/s00402-017-2709-8. Epub 2017 May 9. Arch Orthop Trauma Surg. 2017. PMID: 28488017
-
Synovial C-Reactive Protein is a Useful Adjunct for Diagnosis of Periprosthetic Joint Infection.J Arthroplasty. 2022 Dec;37(12):2437-2443.e1. doi: 10.1016/j.arth.2022.06.016. Epub 2022 Jun 22. J Arthroplasty. 2022. PMID: 35750152 Review.
-
Comparison of periprosthetic joint infection rates in the direct anterior approach and non-anterior approaches to primary total hip arthroplasty: a systematic review and meta-analysis.Hip Int. 2023 Jul;33(4):633-639. doi: 10.1177/11207000221129216. Epub 2022 Oct 10. Hip Int. 2023. PMID: 36214269
Cited by
-
A New Graphic Type Differentiation of Cell Account Determination for Distinguishing Acute Periprosthetic Joint Infection from Hemarthrosis.Antibiotics (Basel). 2022 Sep 21;11(10):1284. doi: 10.3390/antibiotics11101284. Antibiotics (Basel). 2022. PMID: 36289943 Free PMC article.
References
-
- Statistisches Bundesamt . Gesundheit: Fallpauschalenbezogene Krankenhausstatistik (DRG-Statistik) Operationen und Prozeduren der vollstationären Patientinnen und Patienten in Krankenhäusern 2019. Statistisches Bundesamt; Wiesbaden, Germany: 2017.
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
