

GnRH Antagonists with or without Add-Back Therapy: A New Alternative in the Management of Endometriosis?
- PMID: 34768770
- PMCID: PMC8583814
- DOI: 10.3390/ijms222111342
GnRH Antagonists with or without Add-Back Therapy: A New Alternative in the Management of Endometriosis?
Abstract
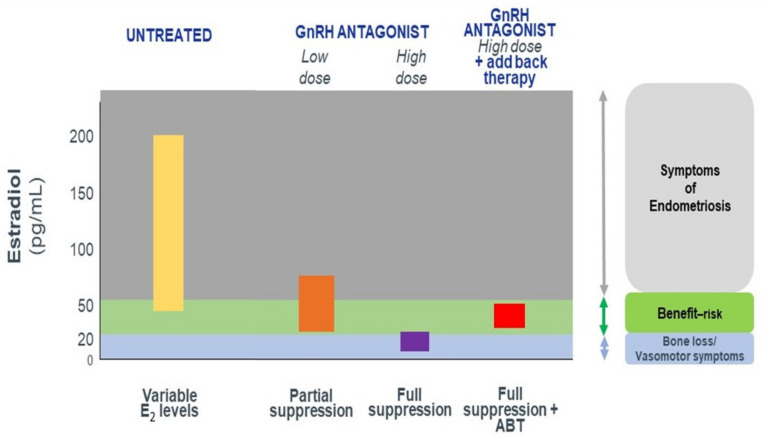
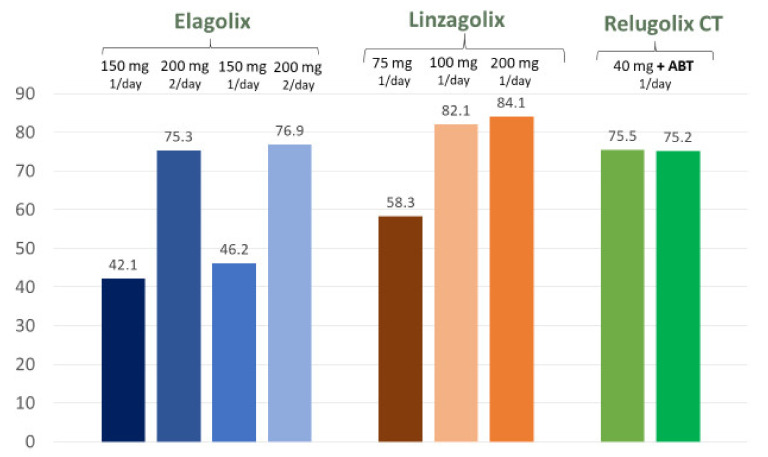
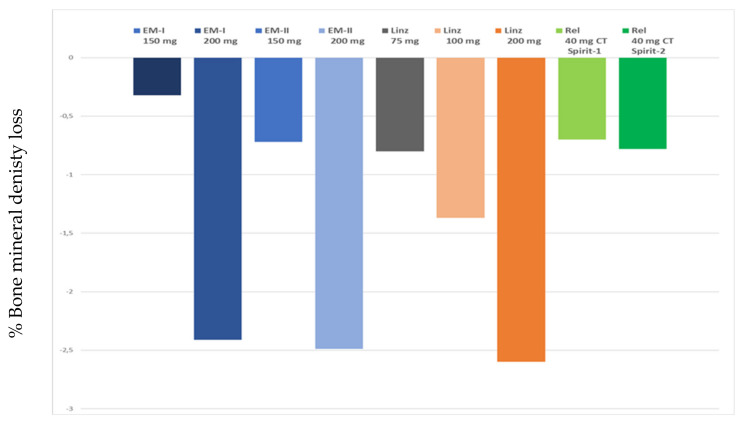
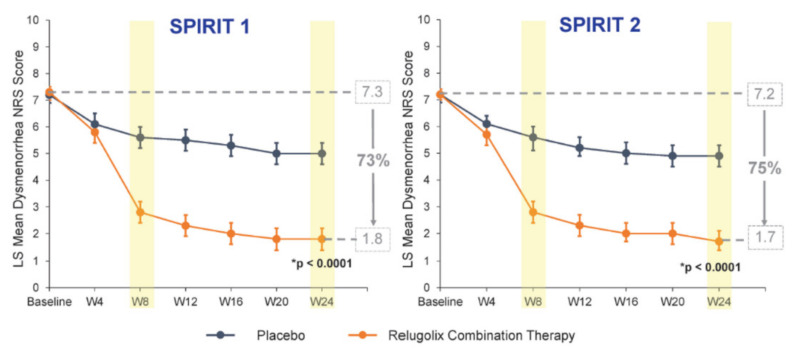
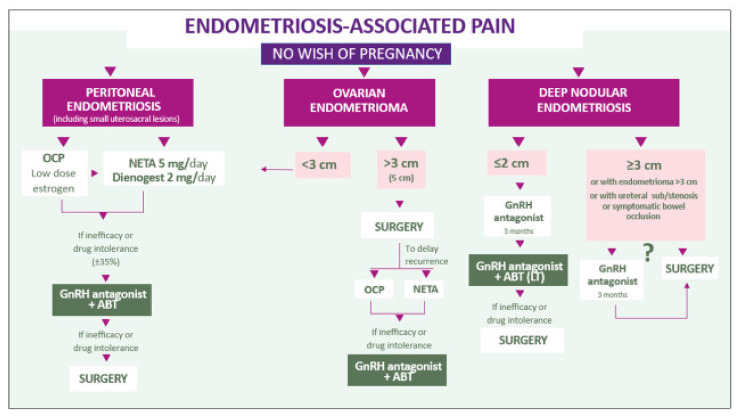
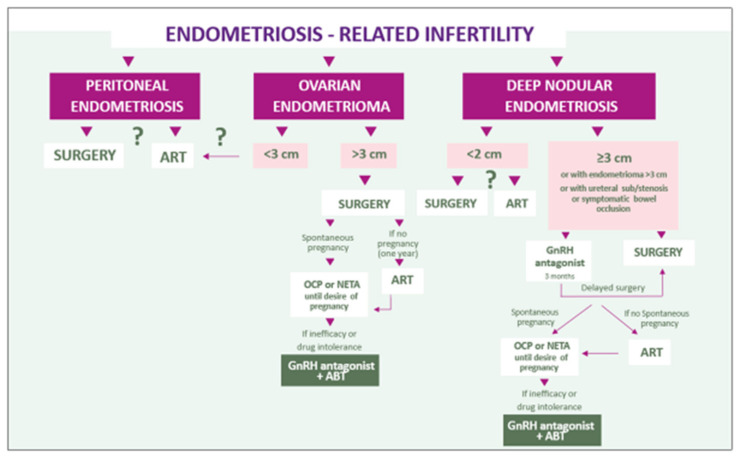
To evaluate the effectiveness of a new class of medical drugs, namely oral gonadotropin-releasing hormone (GnRH) antagonists, in the management of premenopausal women with endometriosis-associated pelvic pain. We reviewed the most relevant papers (n = 27) on the efficacy of new medical alternatives (oral GnRH antagonists) as therapy for endometriosis. We first briefly summarized the concept of progesterone resistance and established that oral contraceptives and progestogens work well in two-thirds of women suffering from endometriosis. Since clinical evidence shows that estrogens play a critical role in the pathogenesis of the disease, lowering their levels with oral GnRH antagonists may well prove effective, especially in women who fail to respond to progestogens. There is a need for reliable long-term oral treatment capable of managing endometriosis symptoms, taking into consideration both the main symptoms and phenotype of the disease. Published studies reviewed and discussed here confirm the efficacy of GnRH antagonists. There is a place for GnRH antagonists in the management of symptomatic endometriosis. Novel algorithms that take into account the different phenotypes are proposed.
Keywords: GnRH antagonist; add-back therapy; dysmenorrhea; elagolix; endometriosis; linzagolix; pelvic pain; progesterone resistance; relugolix.
Conflict of interest statement
Jacques Donnez is member of the Scientific Advisory Board of ObsEva and PregLem. Marie Madeleine Dolmans has nothing to disclose.
Figures
Similar articles
-
Oral GnRH Antagonists in Combination with Estradiol and Norethindrone Acetate for Pain Relief Associated with Endometriosis: A Review of Evidence of a Novel Class of Hormonal Agents.Int J Womens Health. 2024 Feb 27;16:309-321. doi: 10.2147/IJWH.S442357. eCollection 2024. Int J Womens Health. 2024. PMID: 38435758 Free PMC article. Review.
-
Profile of Linzagolix in the Management of Endometriosis, Including Design, Development and Potential Place in Therapy: A Narrative Review.Drug Des Devel Ther. 2023 Feb 8;17:369-380. doi: 10.2147/DDDT.S269976. eCollection 2023. Drug Des Devel Ther. 2023. PMID: 36789095 Free PMC article. Review.
-
Endometriosis and Medical Therapy: From Progestogens to Progesterone Resistance to GnRH Antagonists: A Review.J Clin Med. 2021 Mar 5;10(5):1085. doi: 10.3390/jcm10051085. J Clin Med. 2021. PMID: 33807739 Free PMC article. Review.
-
Update on the management of endometriosis-associated pain in France.J Gynecol Obstet Hum Reprod. 2023 Nov;52(9):102664. doi: 10.1016/j.jogoh.2023.102664. Epub 2023 Sep 3. J Gynecol Obstet Hum Reprod. 2023. PMID: 37669732
-
Research development of a new GnRH antagonist (Elagolix) for the treatment of endometriosis: a review of the literature.Arch Gynecol Obstet. 2017 Apr;295(4):827-832. doi: 10.1007/s00404-017-4328-6. Epub 2017 Mar 3. Arch Gynecol Obstet. 2017. PMID: 28255765 Review.
Cited by
-
Efficacy and safety of oral gonadotropin-releasing hormone antagonists in moderate-to-severe endometriosis-associated pain: a systematic review and network meta-analysis.Arch Gynecol Obstet. 2023 Oct;308(4):1047-1056. doi: 10.1007/s00404-022-06862-0. Epub 2023 Jan 19. Arch Gynecol Obstet. 2023. PMID: 36656435 Free PMC article.
-
Development and Application of a Physiologically Based Pharmacokinetic Model for Elagolix in the Adult and Adolescent Population.Clin Pharmacokinet. 2024 Sep;63(9):1357-1370. doi: 10.1007/s40262-024-01402-2. Epub 2024 Jul 26. Clin Pharmacokinet. 2024. PMID: 39060899
-
Oral GnRH Antagonists in Combination with Estradiol and Norethindrone Acetate for Pain Relief Associated with Endometriosis: A Review of Evidence of a Novel Class of Hormonal Agents.Int J Womens Health. 2024 Feb 27;16:309-321. doi: 10.2147/IJWH.S442357. eCollection 2024. Int J Womens Health. 2024. PMID: 38435758 Free PMC article. Review.
-
Emerging Drug Targets for Endometriosis.Biomolecules. 2022 Nov 8;12(11):1654. doi: 10.3390/biom12111654. Biomolecules. 2022. PMID: 36359004 Free PMC article. Review.
-
Endometriosis: An Inflammatory Disease That Requires New Therapeutic Options.Int J Mol Sci. 2022 Jan 28;23(3):1518. doi: 10.3390/ijms23031518. Int J Mol Sci. 2022. PMID: 35163463 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
