

Pathophysiological Molecular Mechanisms of Obesity: A Link between MAFLD and NASH with Cardiovascular Diseases
- PMID: 34769060
- PMCID: PMC8583943
- DOI: 10.3390/ijms222111629
Pathophysiological Molecular Mechanisms of Obesity: A Link between MAFLD and NASH with Cardiovascular Diseases
Abstract
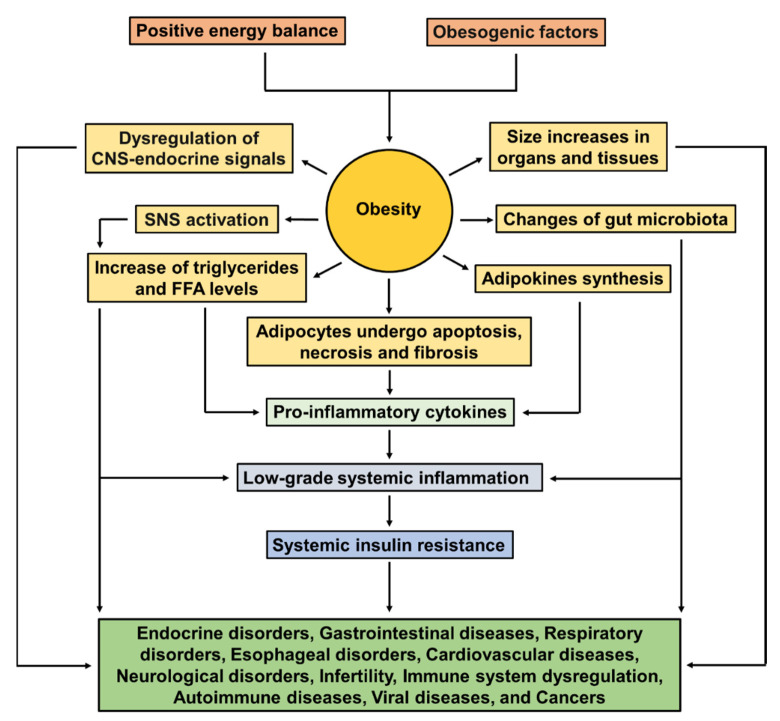
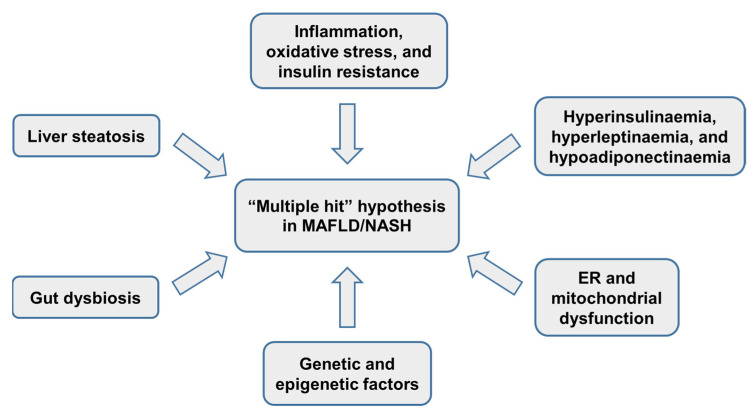
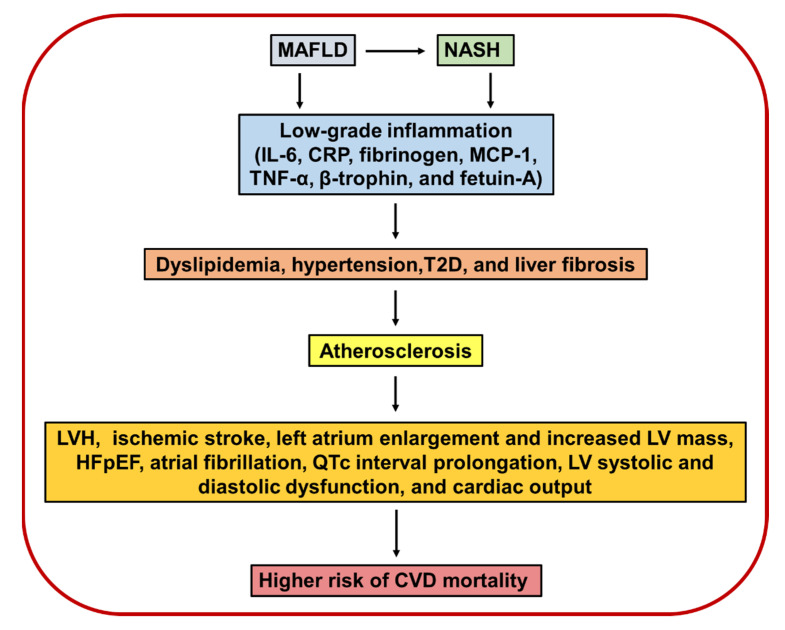
Obesity is now a worldwide epidemic ensuing an increase in comorbidities' prevalence, such as insulin resistance, type 2 diabetes (T2D), metabolic dysfunction-associated fatty liver disease (MAFLD), nonalcoholic steatohepatitis (NASH), hypertension, cardiovascular disease (CVD), autoimmune diseases, and some cancers, CVD being one of the main causes of death in the world. Several studies provide evidence for an association between MAFLD and atherosclerosis and cardio-metabolic disorders, including CVDs such as coronary heart disease and stroke. Therefore, the combination of MAFLD/NASH is associated with vascular risk and CVD progression, but the underlying mechanisms linking MAFLD/NASH and CVD are still under investigation. Several underlying mechanisms may probably be involved, including hepatic/systemic insulin resistance, atherogenic dyslipidemia, hypertension, as well as pro-atherogenic, pro-coagulant, and pro-inflammatory mediators released from the steatotic/inflamed liver. MAFLD is strongly associated with insulin resistance, which is involved in its pathogenesis and progression to NASH. Insulin resistance is a major cardiovascular risk factor in subjects without diabetes. However, T2D has been considered the most common link between MAFLD/NASH and CVD. This review summarizes the evidence linking obesity with MAFLD, NASH, and CVD, considering the pathophysiological molecular mechanisms involved in these diseases. We also discuss the association of MAFLD and NASH with the development and progression of CVD, including structural and functional cardiac alterations, and pharmacological strategies to treat MAFLD/NASH and cardiovascular prevention.
Keywords: cardiovascular diseases; comorbidities of obesity; insulin resistance; metabolic dysfunction-associated fatty liver disease; nonalcoholic steatohepatitis; obesity; pharmacological strategies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Eslam M., Newsome P.N., Sarin S.K., Anstee Q.M., Targher G., Romero-Gomez M., Zelber-Sagi S., Wai-Sun Wong V., Dufour J.F., Schattenberg J.M., et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020;73:202–209. doi: 10.1016/j.jhep.2020.03.039. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
