

Diagnostic Accuracy of Cystic Lesions Using a Pre-Programmed Low-Dose and Standard-Dose Dental Cone-Beam Computed Tomography Protocol: An Ex Vivo Comparison Study
- PMID: 34770710
- PMCID: PMC8588416
- DOI: 10.3390/s21217402
Diagnostic Accuracy of Cystic Lesions Using a Pre-Programmed Low-Dose and Standard-Dose Dental Cone-Beam Computed Tomography Protocol: An Ex Vivo Comparison Study
Abstract
Background: This study aimed to analyze the diagnostic reliability of radiographic assessment of cystic lesions using a pre-set, manufacturer-specific, low-dose mode compared to a standard-dose dental cone-beam computed tomography (CBCT) imaging protocol.
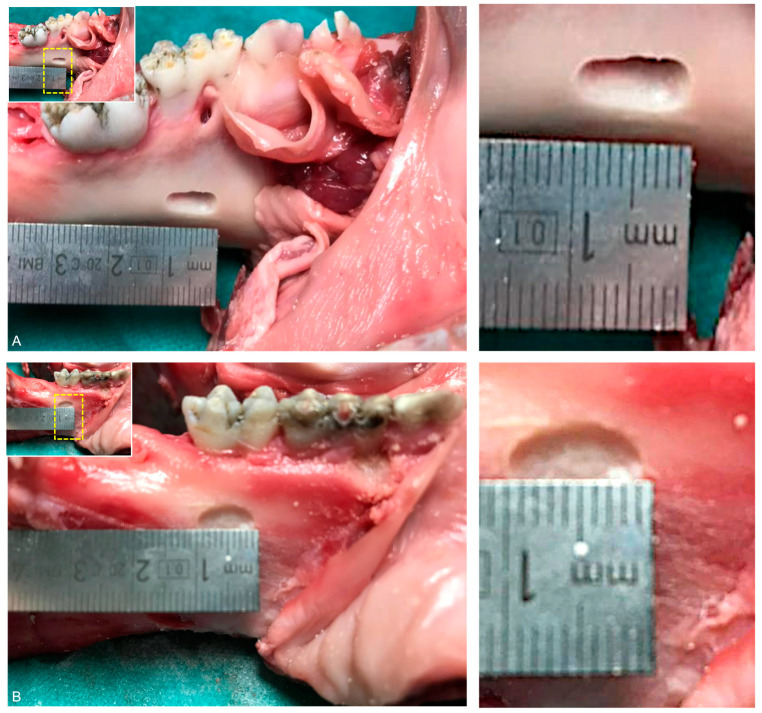
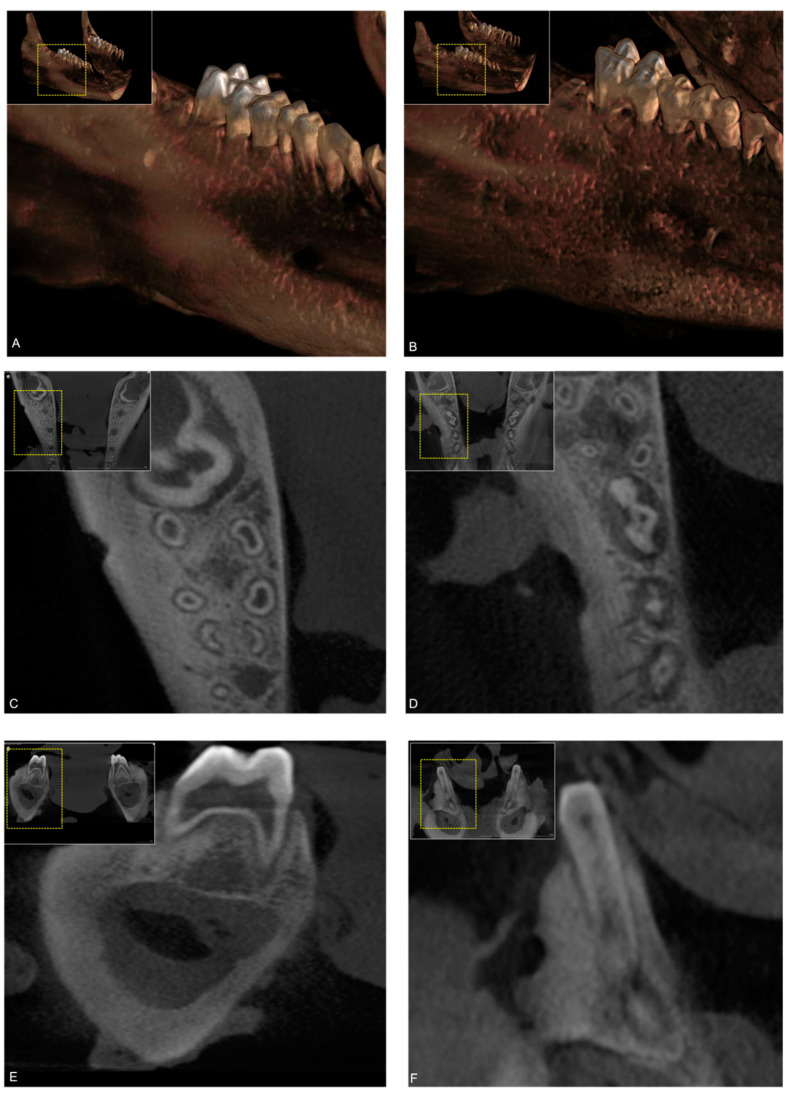
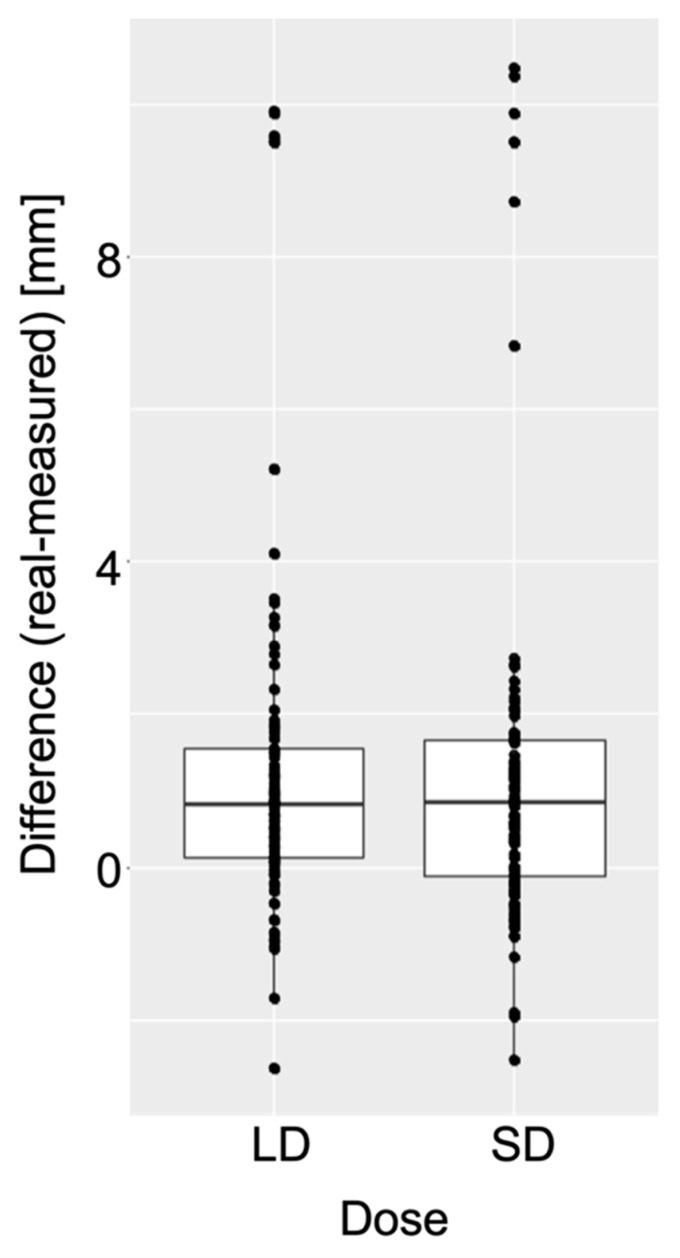
Methods: Forty pig mandible models were prepared with cystic lesions and underwent both CBCT protocols on an Orthophos SL Unit (Dentsply-Sirona, Bensheim, Germany). Qualitative and quantitative analysis of CBCT data was performed by twelve investigators independently in SIDEXIS 4 (Dentsply-Sirona) using a trial-specific digital examination software tool. Thereby, the effect of the two dose types on overall detectability rate, the visibility on a scale of 1 (very low) to 10 (very high) and the difference between measured radiographic and actual lesion size was assessed.
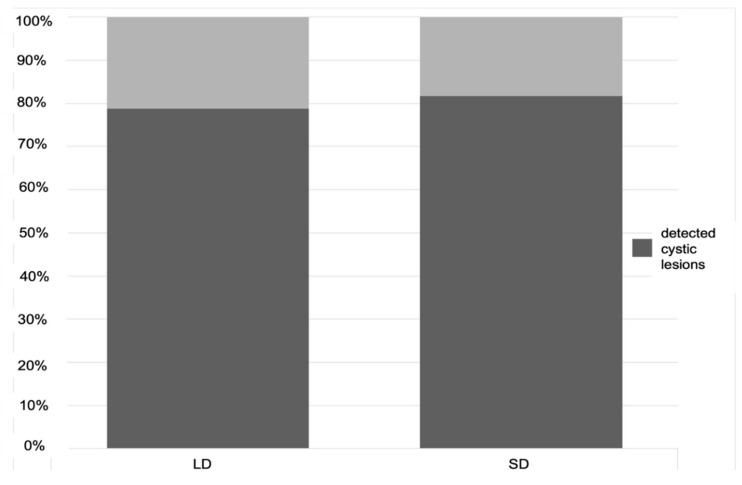
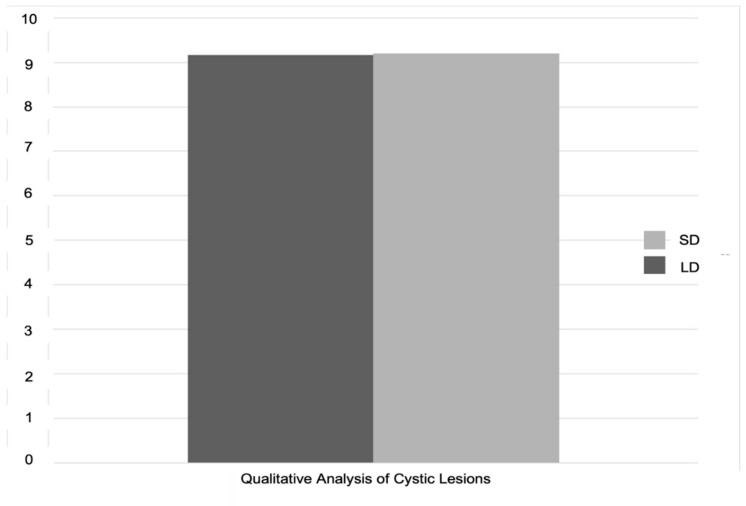
Results: Low-dose CBCT imaging showed no significant differences considering detectability (78.8% vs. 81.6%) and visibility (9.16 vs. 9.19) of cystic lesions compared to the standard protocol. Both imaging protocols performed very similarly in lesion size assessment, with an apparent underestimation of the actual size.
Conclusion: Low-dose protocols providing confidential diagnostic evaluation with an improved benefit-risk ratio according to the ALADA principle could become a promising alternative as a primary diagnostic tool as well as for radiological follow-up in the treatment of cystic lesions.
Keywords: cone-beam computed tomography; cystic lesion; low dose protocols; low-dose cone-beam computed tomography; oral anatomy; oral surgery.
Conflict of interest statement
The authors declare no conflict of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Comparison of Geometric Accuracy of Low-Dose and Standard-Dose Dental CBCT Imaging Protocols in CAD/CAM-Guided Dental Implant Surgery.Int J Oral Maxillofac Implants. 2023 March-April;38(2):287-294. doi: 10.11607/jomi.9851. Int J Oral Maxillofac Implants. 2023. PMID: 36525261
-
Comparison of subjective image analysis and effective dose between low-dose cone-beam computed tomography machines.Dentomaxillofac Radiol. 2023 Jan;52(2):20220176. doi: 10.1259/dmfr.20220176. Epub 2022 Oct 24. Dentomaxillofac Radiol. 2023. PMID: 36168973 Free PMC article.
-
Predictability and image quality of low-dose cone-beam computed tomography in computer-guided implantology: An experimental study.J Dent. 2021 Sep;112:103744. doi: 10.1016/j.jdent.2021.103744. Epub 2021 Jul 9. J Dent. 2021. PMID: 34252488
-
Novel low-dose protocols using cone beam computed tomography in dental medicine: a review focusing on indications, limitations, and future possibilities.Clin Oral Investig. 2019 Jun;23(6):2573-2581. doi: 10.1007/s00784-019-02907-y. Epub 2019 Apr 25. Clin Oral Investig. 2019. PMID: 31025192 Review.
-
Accuracy of linear measurements for implant planning based on low-dose cone beam CT protocols: a systematic review and meta-analysis.Dentomaxillofac Radiol. 2024 Apr 29;53(4):207-221. doi: 10.1093/dmfr/twae007. Dentomaxillofac Radiol. 2024. PMID: 38429951 Free PMC article.
Cited by
-
New Frontier in Advanced Dentistry: CBCT, Intraoral Scanner, Sensors, and Artificial Intelligence in Dentistry.Sensors (Basel). 2022 Apr 12;22(8):2942. doi: 10.3390/s22082942. Sensors (Basel). 2022. PMID: 35458927 Free PMC article.
-
Imaging in Third Molar Surgery: A Clinical Update.J Clin Med. 2023 Dec 14;12(24):7688. doi: 10.3390/jcm12247688. J Clin Med. 2023. PMID: 38137758 Free PMC article. Review.
-
Use of a Resorbable Magnesium Membrane for Bone Regeneration After Large Radicular Cyst Removal: A Clinical Case Report.Healthcare (Basel). 2025 May 6;13(9):1068. doi: 10.3390/healthcare13091068. Healthcare (Basel). 2025. PMID: 40361846 Free PMC article.
-
Clinical, Radiological, and Pathological Diagnosis of Fibro-Osseous Lesions of the Oral and Maxillofacial Region: A Retrospective Study.Diagnostics (Basel). 2022 Jan 19;12(2):238. doi: 10.3390/diagnostics12020238. Diagnostics (Basel). 2022. PMID: 35204329 Free PMC article.
-
Accuracy of formula-based volume and image segmentation-based volume in calculation of preoperative cystic jaw lesions' volume.Oral Radiol. 2024 Apr;40(2):259-268. doi: 10.1007/s11282-023-00731-5. Epub 2023 Dec 19. Oral Radiol. 2024. PMID: 38112919 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
