

Predict Early Recurrence of Resectable Hepatocellular Carcinoma Using Multi-Dimensional Artificial Intelligence Analysis of Liver Fibrosis
- PMID: 34771487
- PMCID: PMC8582529
- DOI: 10.3390/cancers13215323
Predict Early Recurrence of Resectable Hepatocellular Carcinoma Using Multi-Dimensional Artificial Intelligence Analysis of Liver Fibrosis
Abstract
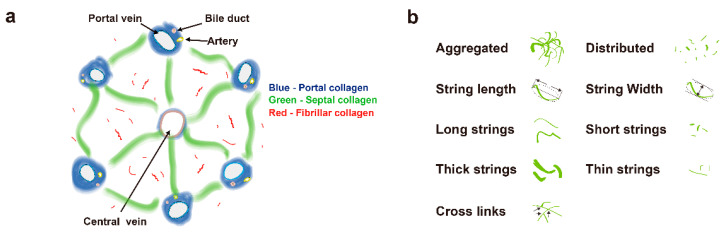
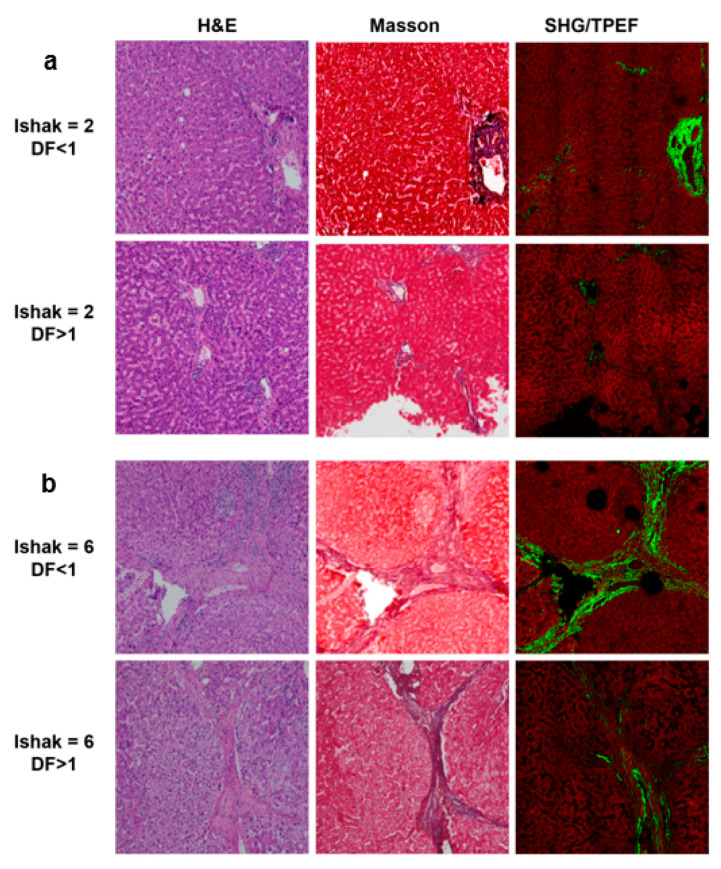
Background: Liver fibrosis is thought to be associated with early recurrence of hepatocellular carcinoma (HCC) after resection. To recognize HCC patients with higher risk of early recurrence, we used a second harmonic generation and two-photon excitation fluorescence (SHG/TPEF) microscopy to create a fully quantitative fibrosis score which is able to predict early recurrence.
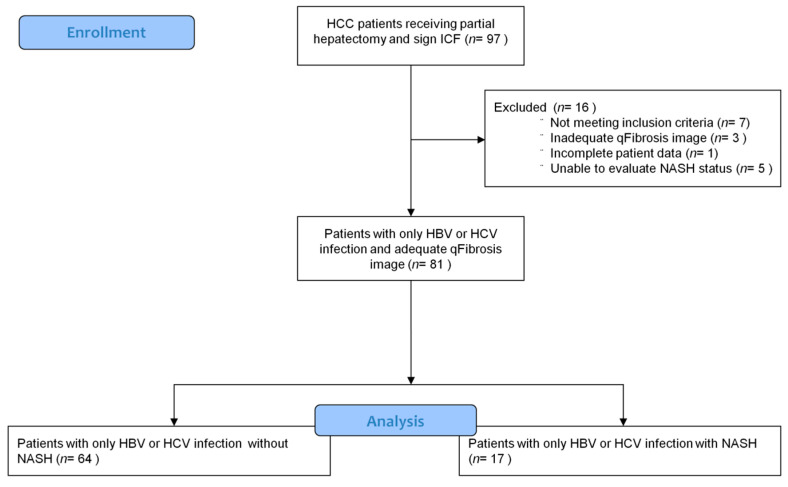
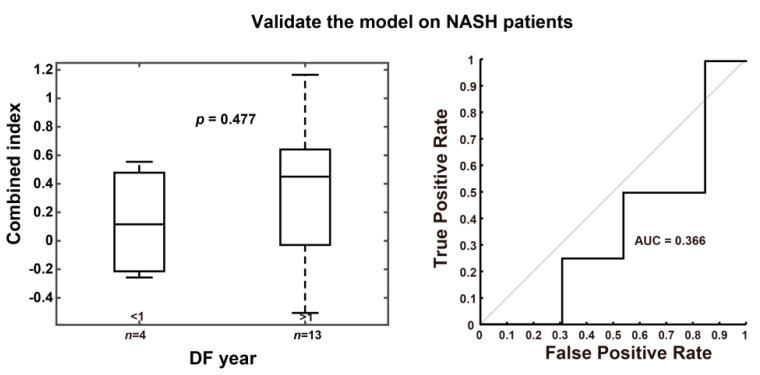
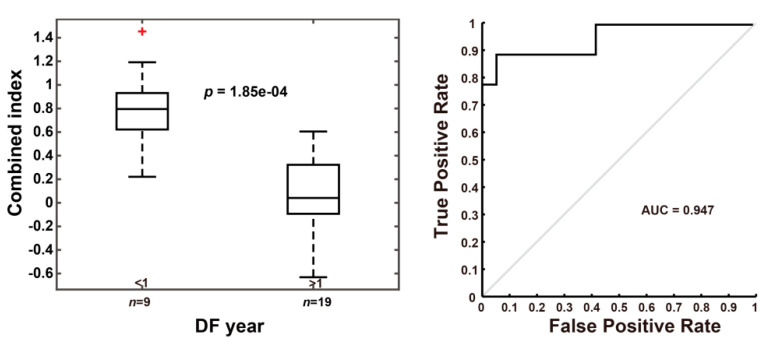
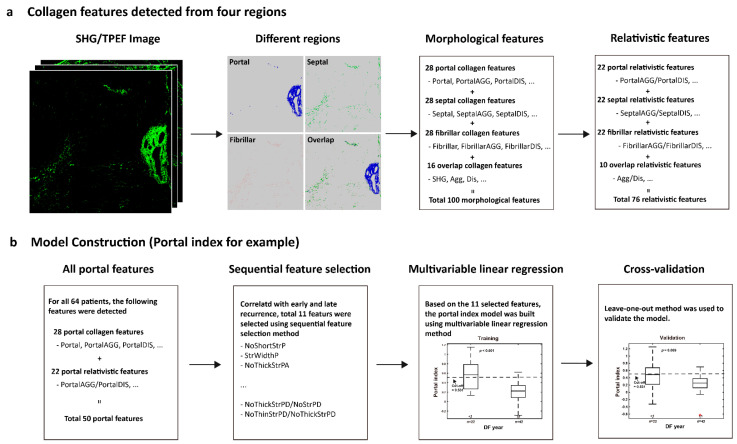
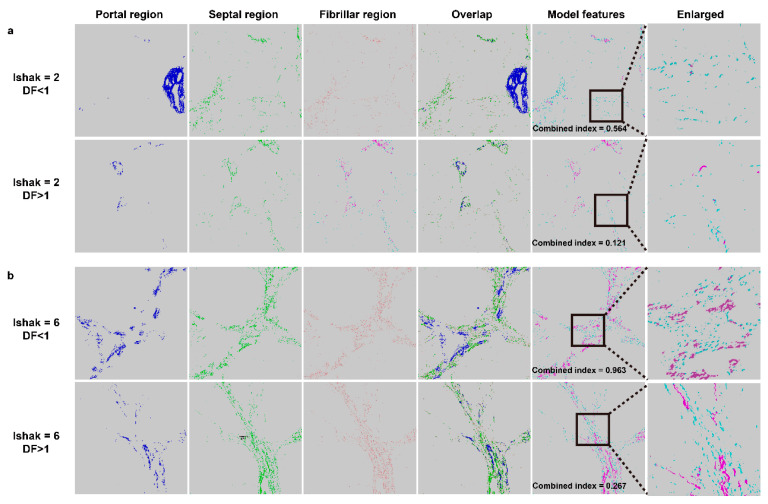
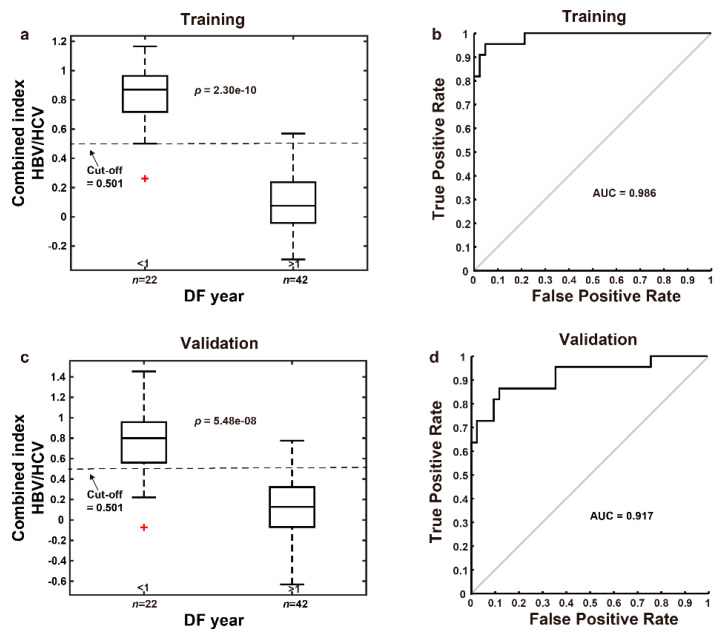
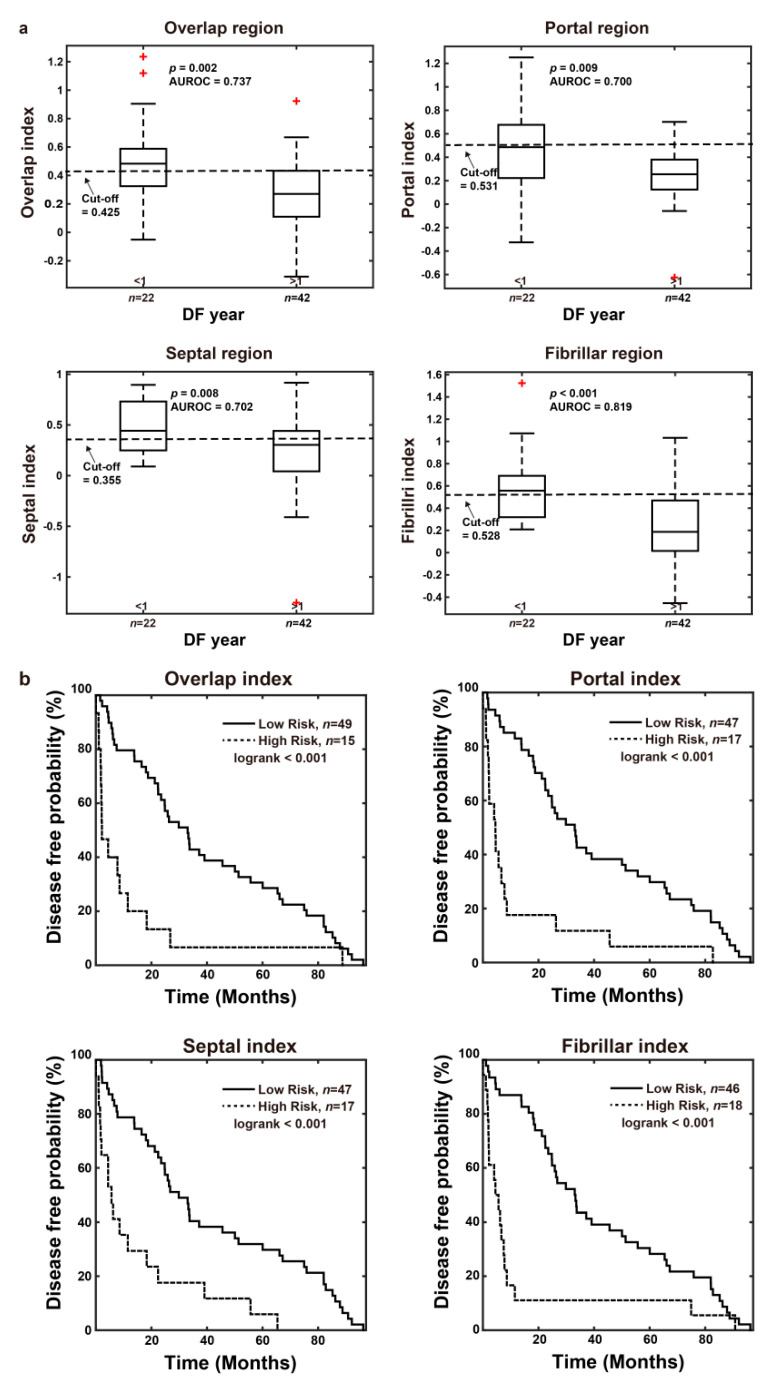
Methods: The study included 81 HCC patients receiving curative intent hepatectomy. Detailed fibrotic features of resected hepatic tissues were obtained by SHG/TPEF microscopy, and we used multi-dimensional artificial intelligence analysis to create a recurrence prediction model "combined index" according to the morphological collagen features of each patient's non-tumor hepatic tissues.
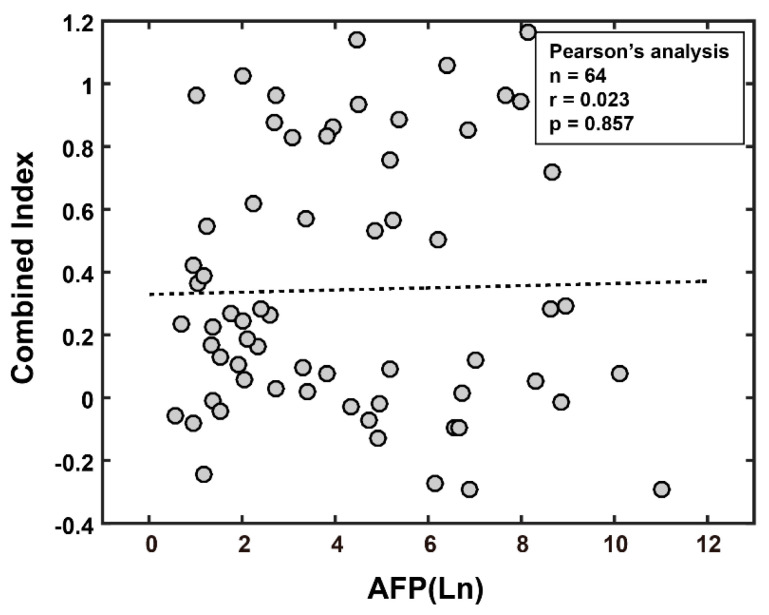
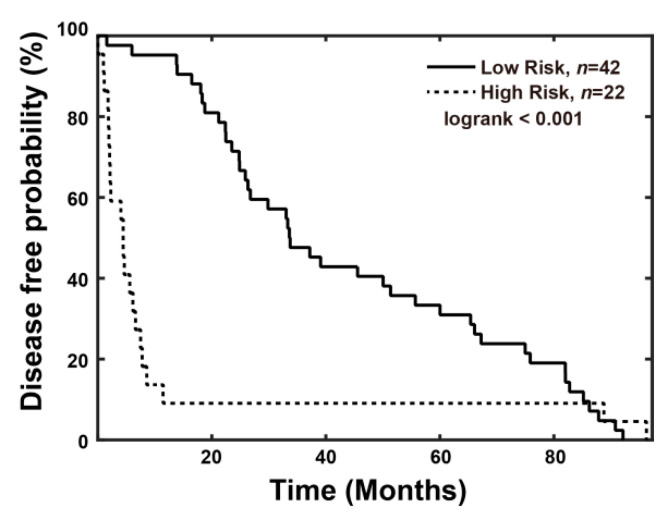
Results: Our results showed that the "combined index" can better predict early recurrence (area under the curve = 0.917, sensitivity = 81.8%, specificity = 90.5%), compared to alpha fetoprotein level (area under the curve = 0.595, sensitivity = 68.2%, specificity = 47.6%). Using a Cox proportional hazards analysis, a higher "combined index" is also a poor prognostic factor of disease-free survival and overall survival.
Conclusions: By integrating multi-dimensional artificial intelligence and SHG/TPEF microscopy, we may locate patients with a higher risk of recurrence, follow these patients more carefully, and conduct further management if needed.
Keywords: SHG/TPEF microscopy; artificial intelligence; hepatocellular carcinoma; liver fibrosis; recurrence.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Shao Y.-Y., Wang S.-Y., Lin S.-M., Chen K.-Y., Tseng J.-H., Ho M.-C., Lee R.-C., Liang P.-C., Liao L.-Y., Huang K.-W., et al. Management consensus guideline for hepatocellular carcinoma: 2020 update on surveillance, diagnosis, and systemic treatment by the Taiwan Liver Cancer Association and the Gastroenterological Society of Taiwan. J. Formos. Med Assoc. 2021;120:1051–1060. doi: 10.1016/j.jfma.2020.10.031. - DOI - PubMed
LinkOut - more resources
Full Text Sources
