

Prognostic value of characteristics of plaque combined with residual syntax score among patients with STEMI undergoing primary PCI: an intravascular optical coherence tomography study
- PMID: 34772417
- PMCID: PMC8588603
- DOI: 10.1186/s12959-021-00329-z
Prognostic value of characteristics of plaque combined with residual syntax score among patients with STEMI undergoing primary PCI: an intravascular optical coherence tomography study
Abstract
Aim: The present study aimed to explore these characteristics, particularly thin-cap fibroatheroma (TCFA), in relation to residual syntax score (rSS) in patients who presented with acute MI.
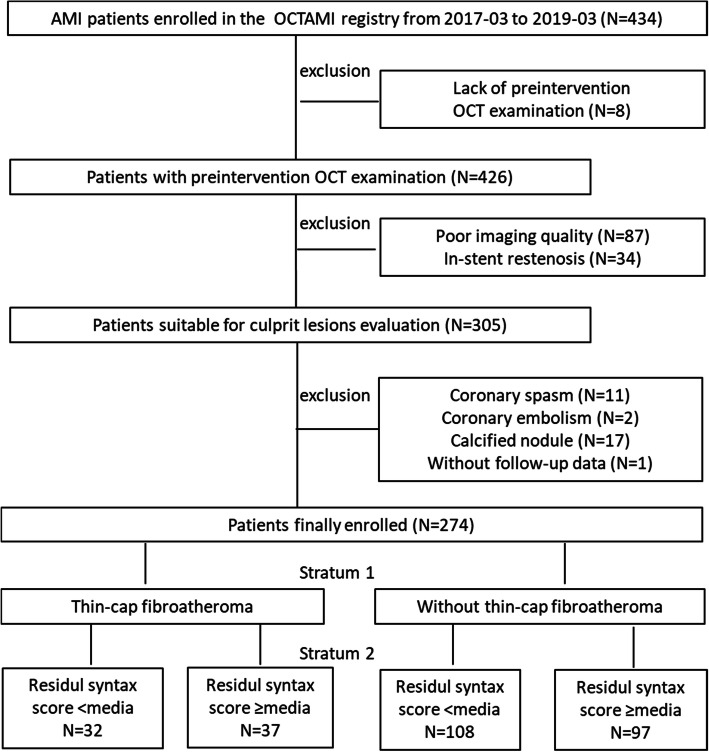
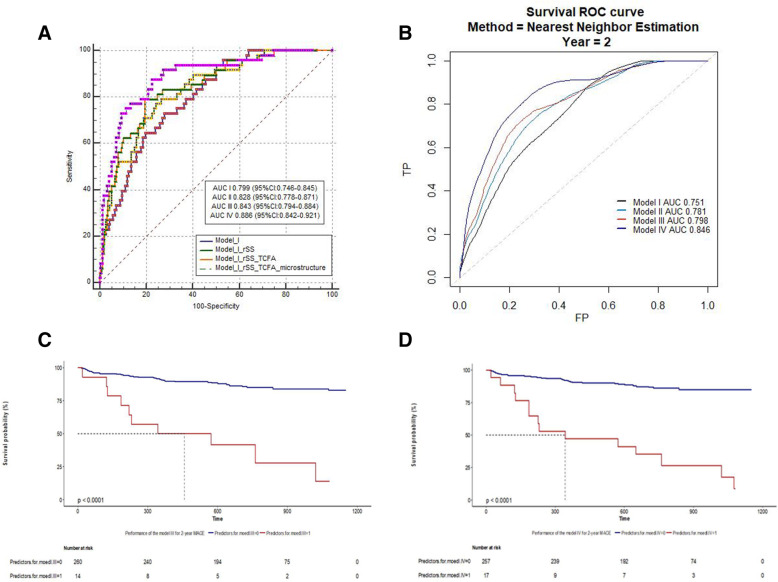
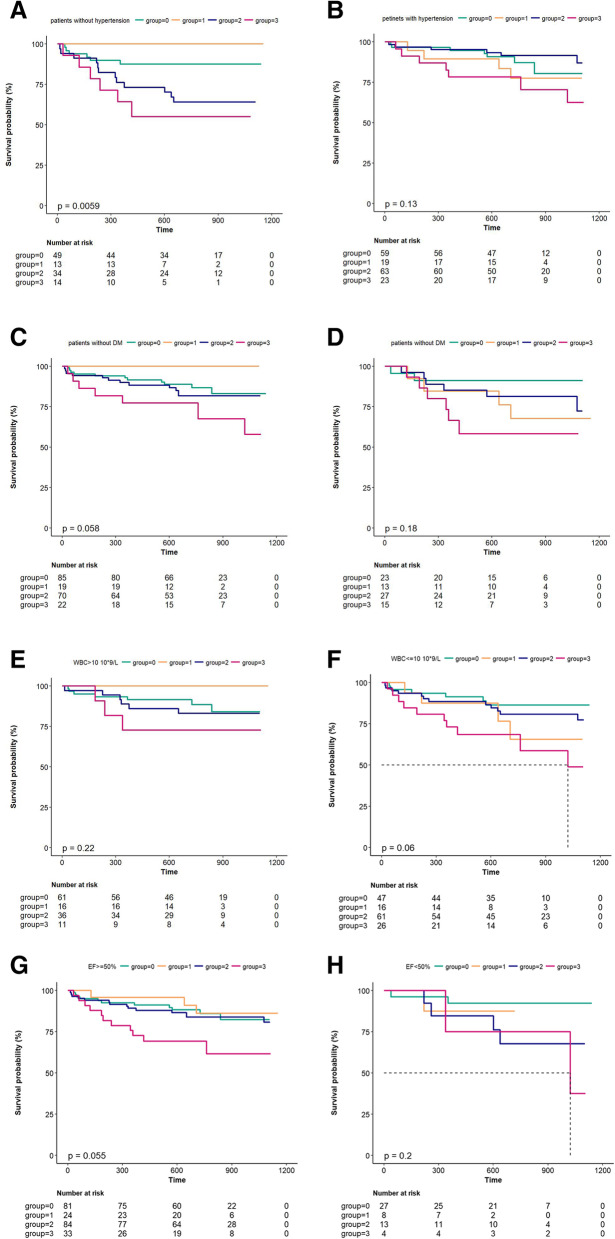
Methods and outcomes: A total of 434 consecutive patients with MI aged ≥18 years who had STEMI underwent primary PCI. Notably, compared with other subgroups, the presence of TCFA in culprit lesions and a higher level of rSS, were significantly associated with MACE. When rSS was divided into three groups, high rSS levels were associated with a higher incidence of MACE, in the subgroups of without TCFA (P = 0.005), plaque erosion (P = 0.045), macrophage infiltration (P = 0.026), and calcification (P = 0.002). AUC of ROC curve was 0.794 and 0.816, whereas the AUC of the survival ROC was 0.798 and 0.846.
Conclusion: The results of this study could be used in clinical practice to support risk stratification.
Trial registration: This study was registered at ClinicalTrials.gov as NCT03593928 .
Keywords: Optical coherence tomography; Prognosis value; Residual syntax score; Thin-cap fibroatheroma.
© 2021. The Author(s).
Conflict of interest statement
Non-financial competing interests.
Non-financial competing interests include family associations, political, religious, academic or any other.
Figures
References
-
- Genereux P, Palmerini T, Caixeta A, et al. Quantification and impact of untreated coronary artery disease after percutaneous coronary intervention: the residual SYNTAX (synergy between PCI with Taxus and cardiac surgery) score. J Am Coll Cardiol. 2012;59:2165–2174. doi: 10.1016/j.jacc.2012.03.010. - DOI - PMC - PubMed
-
- Farooq V, Serruys PW, Bourantas CV, et al. Quantification of incomplete revascularization and its association with five-year mortality in the synergy between percutaneous coronary intervention with taxus and cardiac surgery (SYNTAX) trial validation of the residual SYNTAX score. Circulation. 2013;128:141–151. doi: 10.1161/CIRCULATIONAHA.113.001803. - DOI - PubMed
-
- Park KW, Kang J, Kang SH, et al. The impact of residual coronary lesions on clinical outcomes after percutaneous coronary intervention: residual SYNTAX score after percutaneous coronary intervention in patients from the efficacy of Xience/ Promus versus cypher in rEducing late loss after stENTing (EXCELLENT) registry. Am Heart J. 2014;167:384–92.e5. doi: 10.1016/j.ahj.2013.09.015. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
