

Do health policies address the availability, accessibility, acceptability, and quality of human resources for health? Analysis over three decades of National Health Policy of India
- PMID: 34774088
- PMCID: PMC8590377
- DOI: 10.1186/s12960-021-00681-1
Do health policies address the availability, accessibility, acceptability, and quality of human resources for health? Analysis over three decades of National Health Policy of India
Abstract
Background: Human Resources for Health (HRH) are crucial for improving health services coverage and population health outcomes. The World Health Organisation (WHO) promotes countries to formulate holistic policies that focus on four HRH dimensions-availability, accessibility, acceptability, and quality (AAAQ). The status of these dimensions and their incorporation in the National Health Policies of India (NHPIs) are not well known.
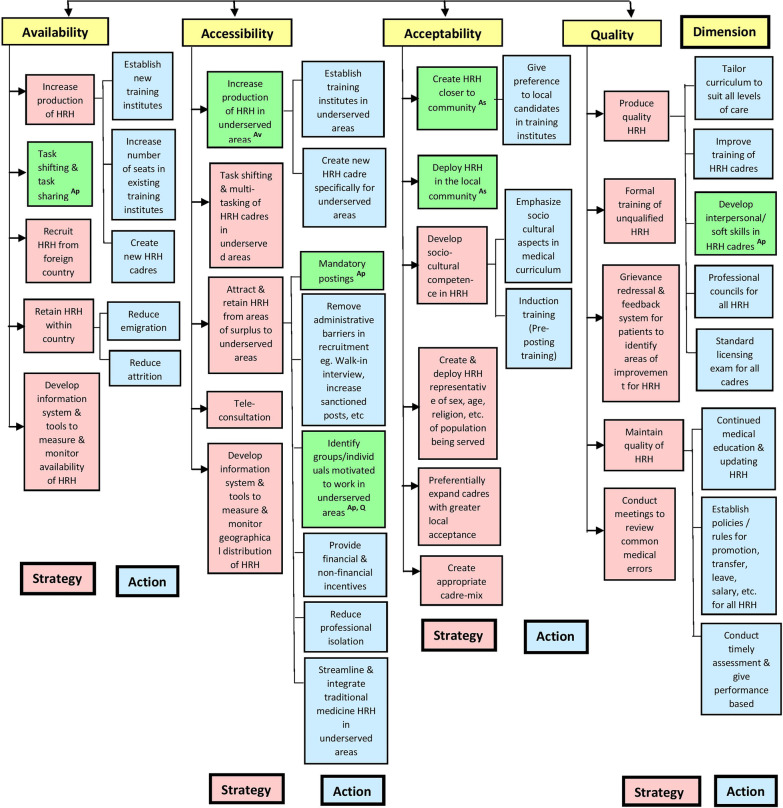
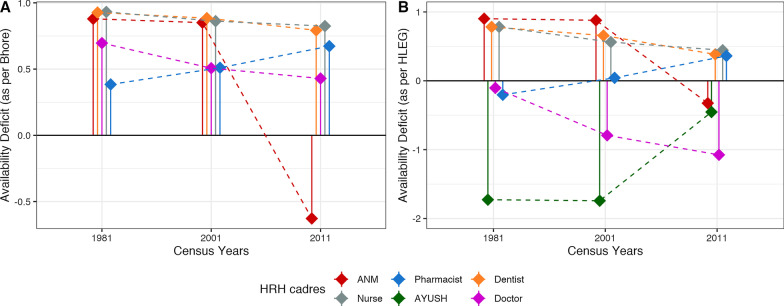
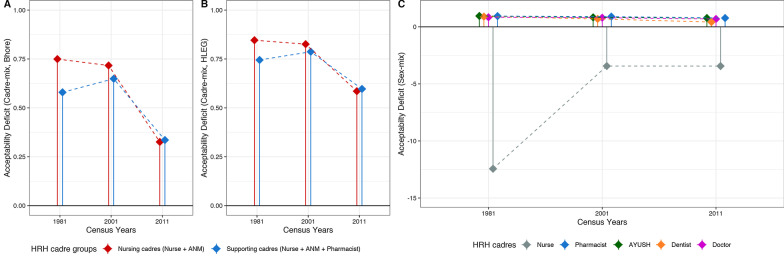
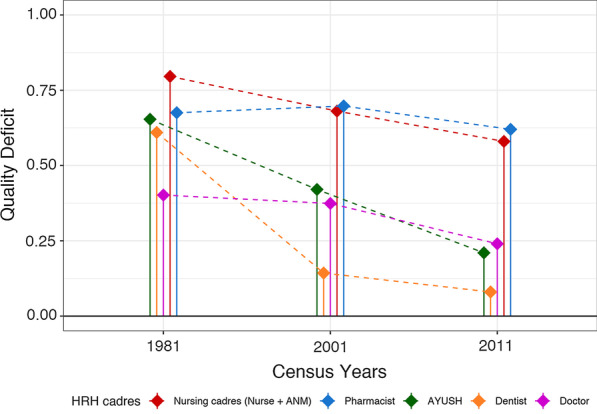
Methods: We created a multilevel framework of strategies and actions directed to improve AAAQ HRH dimensions. HRH-related recommendations of NHPI-1983, 2002, and 2017 were classified according to targeted dimensions and cadres using the framework. We identified the dimensions and cadres focussed by NHPIs using the number of mentions. Furthermore, we introduce a family of dimensionwise deficit indices formulated to assess situational HRH deficiencies for census years (1981, 2001, and 2011) and over-year trends. Finally, we evaluated whether or not the HRH recommendations in NHPIs addressed the deficient cadres and dimensions of the pre-NHPI census years.
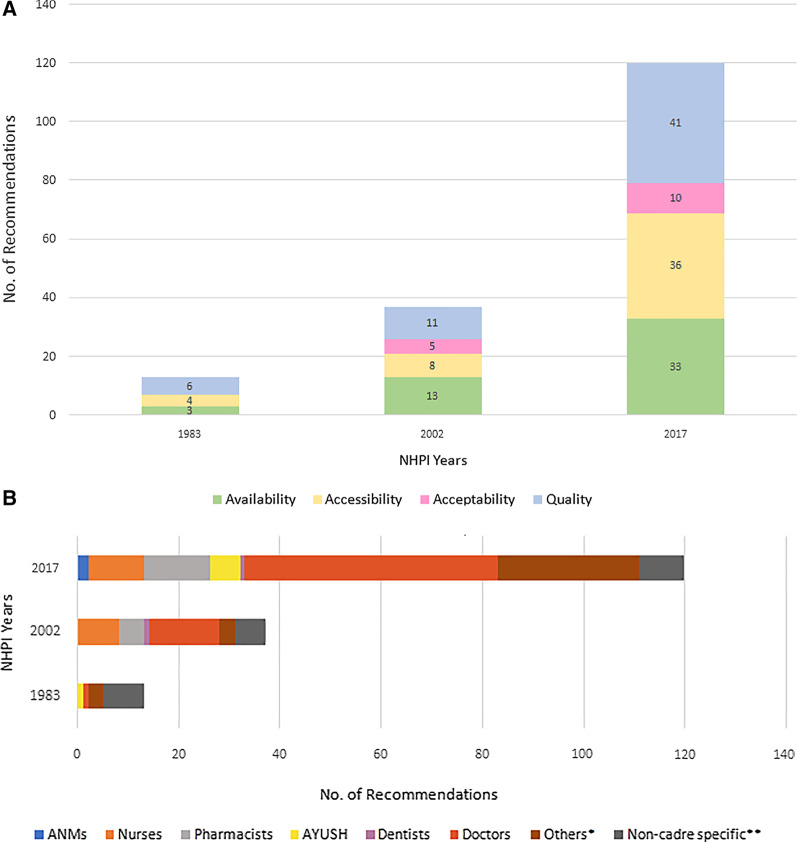
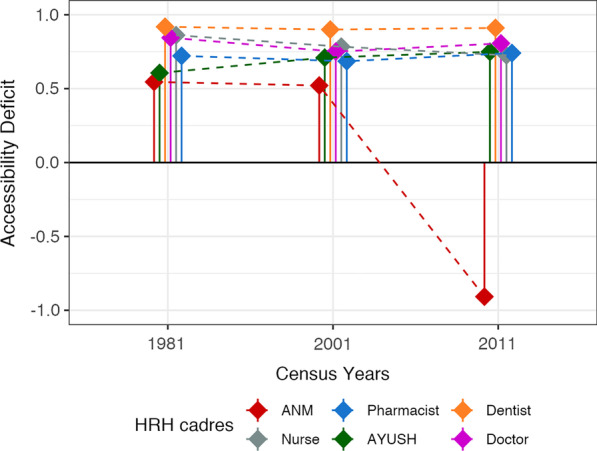
Results: NHPIs focused more on HRH availability and quality compared to accessibility and acceptability. Doctors were prioritized over auxiliary nurses-midwives and pharmacists in terms of total recommendations. AAAQ indices showed deficits in all dimensions for almost all HRH cadres over the years. All deficit indices show a general decreasing trend from 1981 to 2011 except for the accessibility deficit. The recommendations in NHPIs did not correspond to the situational deficits in many instances indicating a policy priority mismatch.
Conclusion: India needs to incorporate AAAQ dimensions in its policies and monitor their progress. The framework and indices-based approach can help identify the gaps between targeted and needed dimensions and cadres for effective HRH strengthening. At the global level, the application of framework and indices will allow a comparison of the strengths and weaknesses of HRH-related policies of various nations.
Keywords: Deficit indices; Health system strengthening; Human Resources for Health; India; National Health Policy; Policy analysis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Human resources for health and universal health coverage: fostering equity and effective coverage.Bull World Health Organ. 2013 Nov 1;91(11):853-63. doi: 10.2471/BLT.13.118729. Bull World Health Organ. 2013. PMID: 24347710 Free PMC article.
-
Implementing a health labour market analysis to address health workforce gaps in a rural region of India.Hum Resour Health. 2022 Jun 4;20(1):50. doi: 10.1186/s12960-022-00749-6. Hum Resour Health. 2022. PMID: 35659250 Free PMC article.
-
Health workforce monitoring in Portugal: Does it support strategic planning and policy-making?Health Policy. 2020 Mar;124(3):303-310. doi: 10.1016/j.healthpol.2019.12.014. Epub 2020 Jan 7. Health Policy. 2020. PMID: 31932075
-
A scoping review of training and deployment policies for human resources for health for maternal, newborn, and child health in rural Africa.Hum Resour Health. 2014 Dec 16;12:72. doi: 10.1186/1478-4491-12-72. Hum Resour Health. 2014. PMID: 25515732 Free PMC article.
-
COVID-19 and human resources for health: analysis of planning, policy responses and actions in Latin American and Caribbean countries.Hum Resour Health. 2023 Mar 14;21(1):21. doi: 10.1186/s12960-023-00795-8. Hum Resour Health. 2023. PMID: 36918895 Free PMC article. Review.
Cited by
-
Type of Findings Generated by the Occupational Therapy Workforce Research Worldwide: Scoping Review and Content Analysis.Int J Environ Res Public Health. 2022 Apr 27;19(9):5307. doi: 10.3390/ijerph19095307. Int J Environ Res Public Health. 2022. PMID: 35564701 Free PMC article.
-
Evaluating the status of the Lancet Commission on Global Surgery indicators for India.Lancet Reg Health Southeast Asia. 2023 Apr 5;13:100178. doi: 10.1016/j.lansea.2023.100178. eCollection 2023 Jun. Lancet Reg Health Southeast Asia. 2023. PMID: 37383563 Free PMC article. Review.
-
Maternity Care Experiences of African-Born Women Living in Melbourne, Australia: A Qualitative Descriptive Study.J Racial Ethn Health Disparities. 2024 Dec 30. doi: 10.1007/s40615-024-02264-x. Online ahead of print. J Racial Ethn Health Disparities. 2024. PMID: 39739203
-
Prioritization of surgical, obstetric, trauma, and anesthesia care in India over seven decades: A systematic analysis of policy documents.PLOS Glob Public Health. 2023 Jul 31;3(7):e0002084. doi: 10.1371/journal.pgph.0002084. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 37523346 Free PMC article.
-
Physical accessibility, availability, financial affordability, and acceptability of mobile health clinics in remote areas of Saudi Arabia.J Family Med Prim Care. 2023 Sep;12(9):1947-1956. doi: 10.4103/jfmpc.jfmpc_567_23. Epub 2023 Sep 30. J Family Med Prim Care. 2023. PMID: 38024907 Free PMC article.
References
-
- Speybroeck N, Kinfu Y, Dal Poz MR, Evans DB. Reassessing the relationship between human resources for health, intervention coverage and health outcomes. WHO, Geneva: World Health Organization (WHO); 2006 Mar.
-
- United Nations Development Programme. Human resources for health | United Nations Development Programme. https://www.undp-capacitydevelopment-health.org/en/capacities/focus/prog.... Accessed 19 Aug 2021.
-
- World Health Organization (WHO). Framing the health workforce agenda for the Sustainable Development Goals: Biennium report 2016–2017 WHO health workforce. World Health Organization (WHO); 2017.
-
- World Health Organization (WHO). Global strategy on human resources for health: Workforce 2030. World Health Organization (WHO); 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
