

Dexmedetomidine vs. lidocaine for postoperative analgesia in pediatric patients undergoing craniotomy: a protocol for a prospective, randomized, double-blinded, placebo-controlled trial
- PMID: 34774098
- PMCID: PMC8590361
- DOI: 10.1186/s13063-021-05774-9
Dexmedetomidine vs. lidocaine for postoperative analgesia in pediatric patients undergoing craniotomy: a protocol for a prospective, randomized, double-blinded, placebo-controlled trial
Abstract
Background: Postoperative pain is a common problem that occurs in pediatric patients following neurosurgery which may lead to severe complications. Dexmedetomidine is a commonly used adjuvant medicine in craniotomy owing to its sedative, amnestic, analgesic, and neuroprotective properties. Besides, studies suggest that lidocaine has similar effects on sedation, analgesia, and neuroprotection. Both two adjuvants can reduce postoperative pain after neurosurgery in adults. However, it is still unknown whether dexmedetomidine or lidocaine can reduce postoperative pain in children undergoing craniotomy, and if yes, which is a better medicine choice. Therefore, we aimed to compare the effect of dexmedetomidine vs. lidocaine on postoperative pain in pediatric patients after craniotomy.
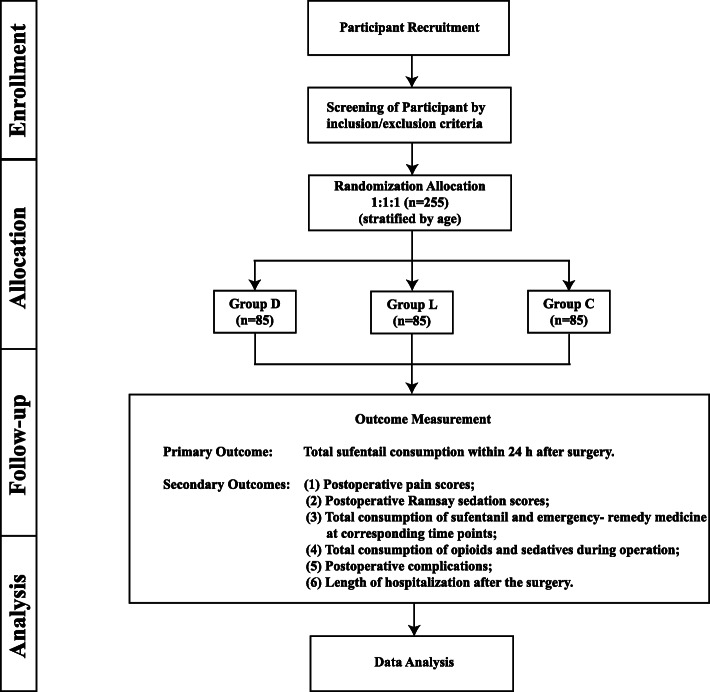
Methods/design: We will perform a randomized (1:1:1), double-blind, placebo-controlled, single-center trial. Children aged 1-12 years scheduled for craniotomy will be eligible for inclusion. The 255 recruited participants will be stratified by age in two strata (1-6 years and 7-12 years), and then each stratum will be equally randomized to three groups: group D (infusion of dexmedetomidine [intervention group]), group L (infusion of lidocaine [intervention group]), and group C (infusion of normal saline [control group]). Patients will be followed up at 1 h, 2 h, 4 h, 24 h, and 48 h after surgery. The primary outcome will be total sufentanil consumption within 24 h after surgery.
Discussion: In this clinical trial, we expect to clarify and compare the postoperative analgesic effect of dexmedetomidine vs. lidocaine infusion on pediatric patients undergoing craniotomy. We believe that the results of this trial will provide more choices for postoperative analgesia for the pediatric population.
Trial registration: Chinese ClinicalTrials.gov ChiCTR1800019411 . Registered on 10 November 2018.
Keywords: Craniotomy; Dexmedetomidine; Lidocaine; Pediatric; Postoperative analgesia.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
References
-
- Dunbar PJ, Visco E, Lam AM. Craniotomy procedures are associated with less analgesic requirements than other surgical procedures. Anesthesia and Analgesia. 1999;88(2):335–340. - PubMed
-
- Flexman AM, Ng JL, Gelb AW. Acute and chronic pain following craniotomy. Curr Opin Anaesthesiol. 2010;23(5):551–557. - PubMed
-
- Gottschalk A, Berkow LC, Stevens RD, Mirski M, Thompson RE, White ED, et al. Prospective evaluation of pain and analgesic use following major elective intracranial surgery. Journal of Neurosurgery. 2007;106(2):210–216. - PubMed
-
- Mordhorst C, Latz B, Kerz T, Wisser G, Schmidt A, Schneider A, et al. Prospective assessment of postoperative pain after craniotomy. J Neurosurg Anesthesiol. 2010;22(3):202–206. - PubMed
-
- Silberstein S, Olesen J, Bousser M, Diener H, Dodick D, First M, et al. International Headache Society. The International Classification of Headache Disorders, (ICHD-II)—revision of criteria for 8.2 medication-overuse headache. Headache. 2005;45(10):1424–1425. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
