

Prone positioning for non-intubated spontaneously breathing patients with acute hypoxaemic respiratory failure: a systematic review and meta-analysis
- PMID: 34774295
- PMCID: PMC8514681
- DOI: 10.1016/j.bja.2021.09.031
Prone positioning for non-intubated spontaneously breathing patients with acute hypoxaemic respiratory failure: a systematic review and meta-analysis
Abstract
Background: Prone positioning in non-intubated spontaneously breathing patients is becoming widely applied in practice alongside noninvasive respiratory support. This systematic review and meta-analysis evaluates the effect, timing, and populations that might benefit from awake proning regarding oxygenation, mortality, and tracheal intubation compared with supine position in hypoxaemic acute respiratory failure.
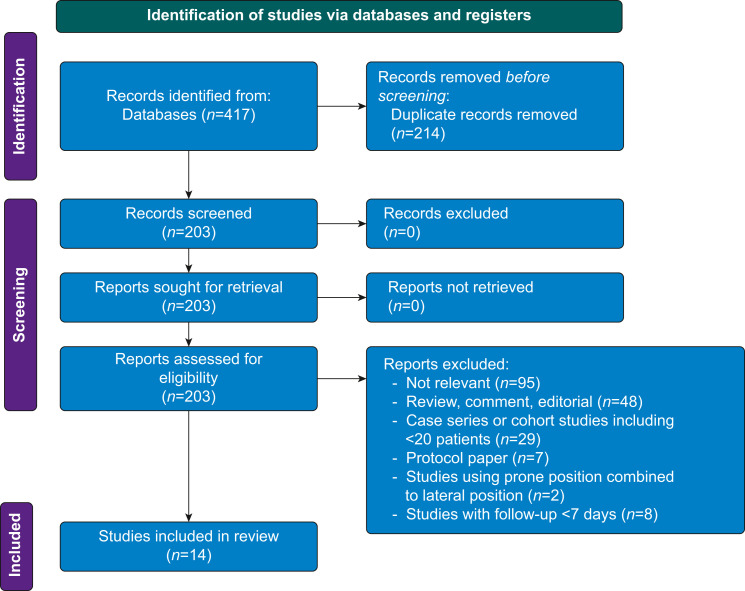
Methods: We conducted a systematic literature search of PubMed/MEDLINE, Cochrane Library, Embase, CINAHL, and BMJ Best Practice until August 2021 (International Prospective Register of Systematic Reviews [PROSPERO] registration: CRD42021250322). Studies included comprise least-wise 20 adult patients with hypoxaemic respiratory failure secondary to acute respiratory distress syndrome or coronavirus disease (COVID-19). Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed, and study quality was assessed using the Newcastle-Ottawa Scale and the Cochrane risk-of-bias tool.
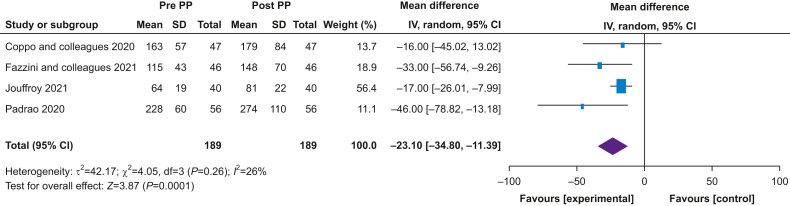
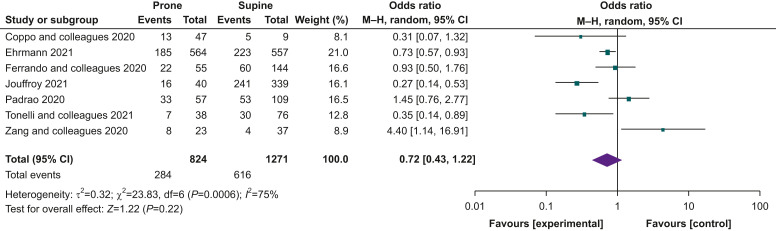
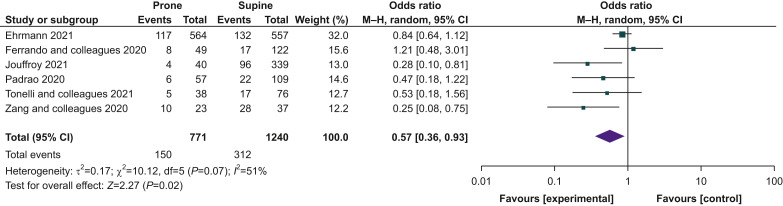
Results: Fourteen studies fulfilled the selection criteria and 2352 patients were included; of those patients, 99% (n=2332/2352) had COVID-19. Amongst 1041 (44%) patients who were placed in the prone position, 1021 were SARS-CoV-2 positive. The meta-analysis revealed significant improvement in the PaO2/FiO2 ratio (mean difference -23.10; 95% confidence interval [CI]: -34.80 to 11.39; P=0.0001; I2=26%) after prone positioning. In patients with COVID-19, lower mortality was found in the group placed in the prone position (150/771 prone vs 391/1457 supine; odds ratio [OR] 0.51; 95% CI: 0.32-0.80; P=0.003; I2=48%), but the tracheal intubation rate was unchanged (284/824 prone vs 616/1271 supine; OR 0.72; 95% CI: 0.43-1.22; P=0.220; I2=75%). Overall proning was tolerated for a median of 4 h (inter-quartile range: 2-16).
Conclusions: Prone positioning can improve oxygenation amongst non-intubated patients with acute hypoxaemic respiratory failure when applied for at least 4 h over repeated daily episodes. Awake proning appears safe, but the effect on tracheal intubation rate and survival remains uncertain.
Keywords: ARDS; COVID-19; SARS-CoV-2; awake prone position; hypoxaemic respiratory failure; noninvasive respiratory support; tracheal intubation.
Crown Copyright © 2021. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
RP is an editor of the
Figures
Comment in
-
Breathing face down.Br J Anaesth. 2022 May;128(5):745-747. doi: 10.1016/j.bja.2022.01.024. Epub 2022 Feb 23. Br J Anaesth. 2022. PMID: 35216817 Free PMC article.
References
-
- Guérin C., Reignier J., Richard J.C., et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. - PubMed
-
- Gattinoni L., Marini J.J., Pesenti A., Quintel M., Mancebo J., Brochard L. The ‘baby lung’ became an adult. Intensive Care Med. 2016;42:663–673. - PubMed
-
- Bamford P., Bentley A., Dean J., Wilson-Baig N. ICS guidance for prone positioning of the conscious COVID patient 2020. https://static1.squarespace.com/static/5e6613a1dc75b87df82b78e1/t/5e99e7... Available from:
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
