

3D Specimen Mapping Expedites Frozen Section Diagnosis of Nonpalpable Ground Glass Opacities
- PMID: 34774493
- PMCID: PMC9188686
- DOI: 10.1016/j.athoracsur.2021.09.069
3D Specimen Mapping Expedites Frozen Section Diagnosis of Nonpalpable Ground Glass Opacities
Abstract
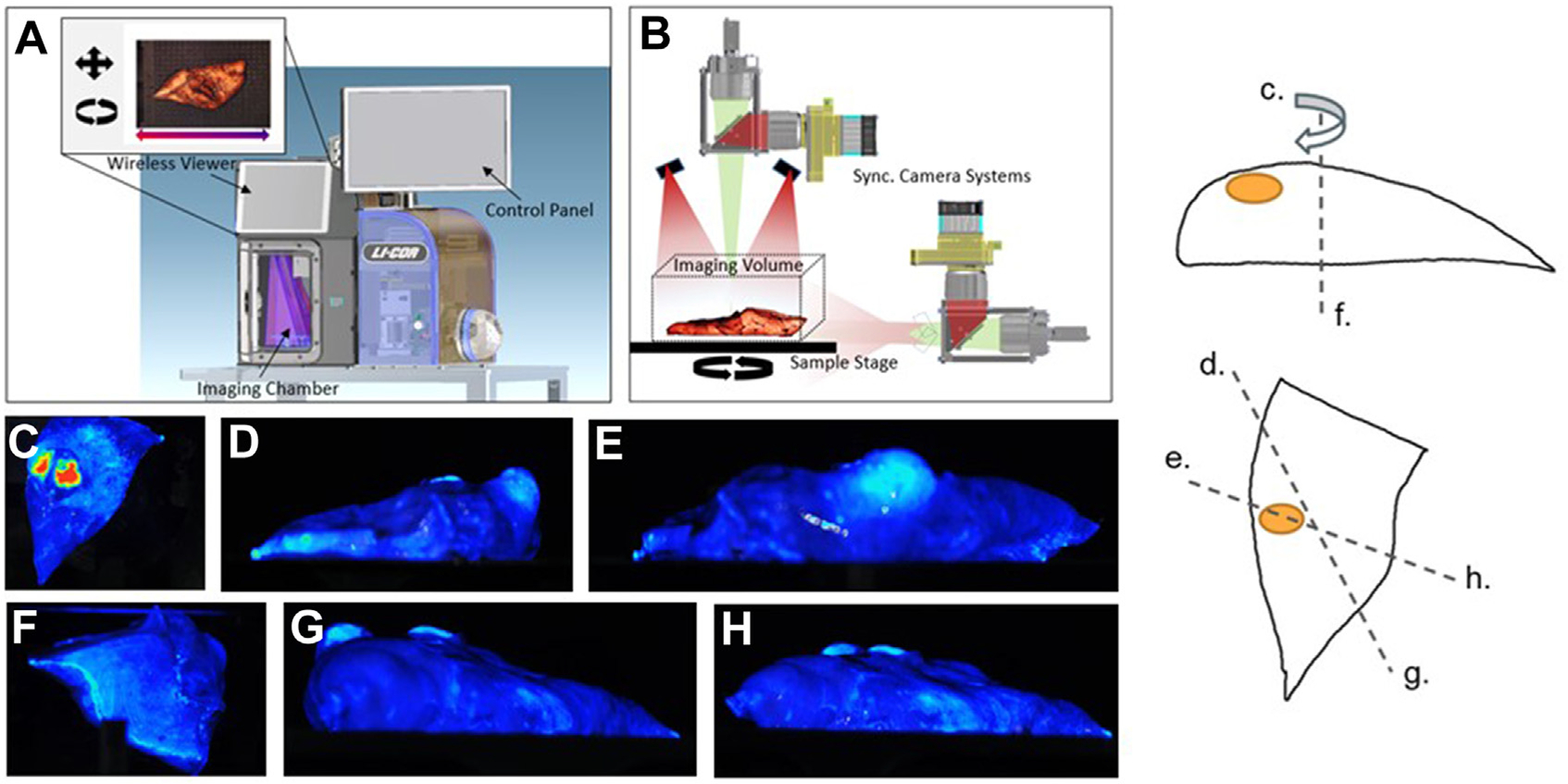
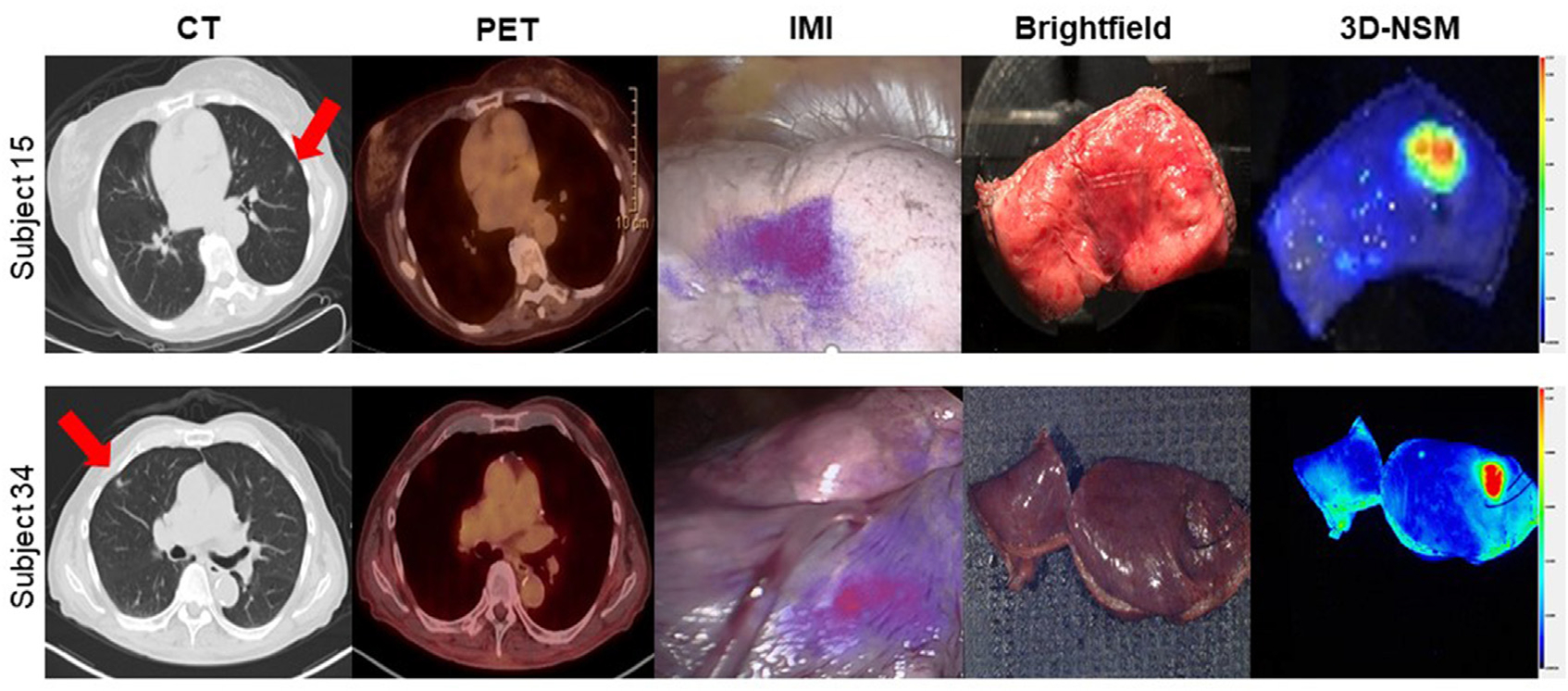
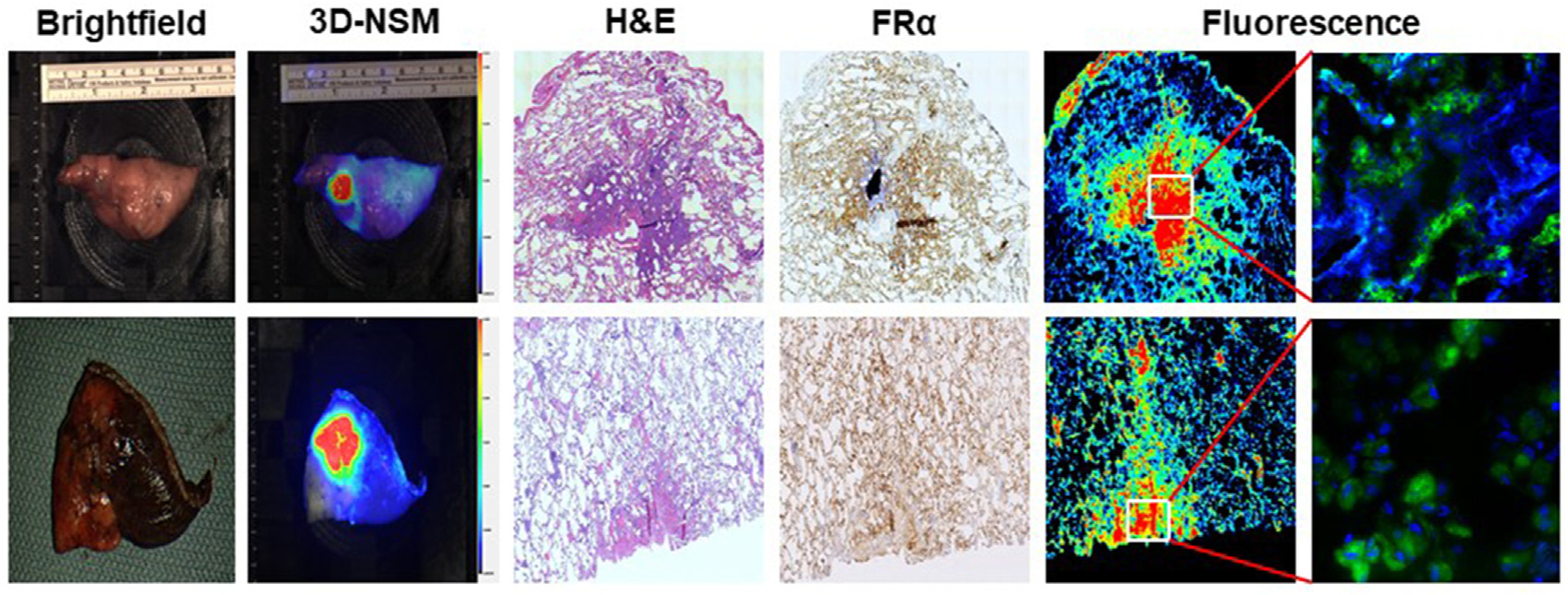
Background: Pulmonary ground glass opacities (GGOs) are early-stage adenocarcinoma spectrum lesions that are not easily palpable. Challenges in localizing GGOs during intraoperative pathology can lead to imprecise diagnoses and additional time under anesthesia. To improve localization of GGOs during frozen section diagnosis, we evaluated a novel technique, 3-dimensional near-infrared specimen mapping (3D-NSM).
Methods: Fifty-five patients with a cT1 GGO were enrolled and received a fluorescent tracer preoperatively. After resection, specimens were inspected to identify lesions. Palpable and nonpalpable nodules underwent 3D-NSM and the area of highest fluorescence was marked with a suture. Time for 3D-NSM, time for frozen section diagnosis, and number of tissue sections examined were recorded. To compare 3D-NSM with standard-of-care techniques, a control cohort of 20 subjects with identical inclusion criteria were enrolled. Specimens did not undergo 3D-NSM and were sent directly to pathology.
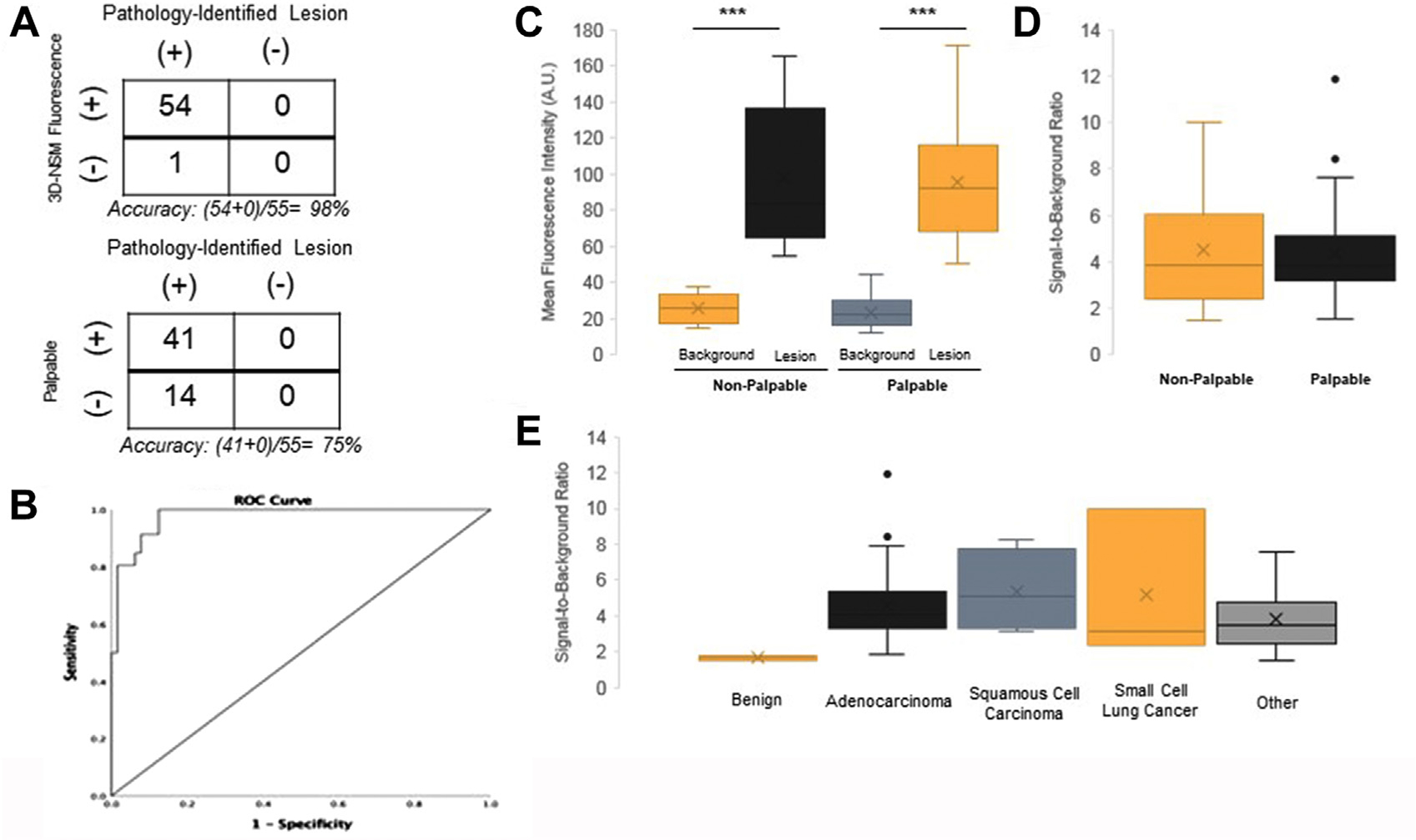
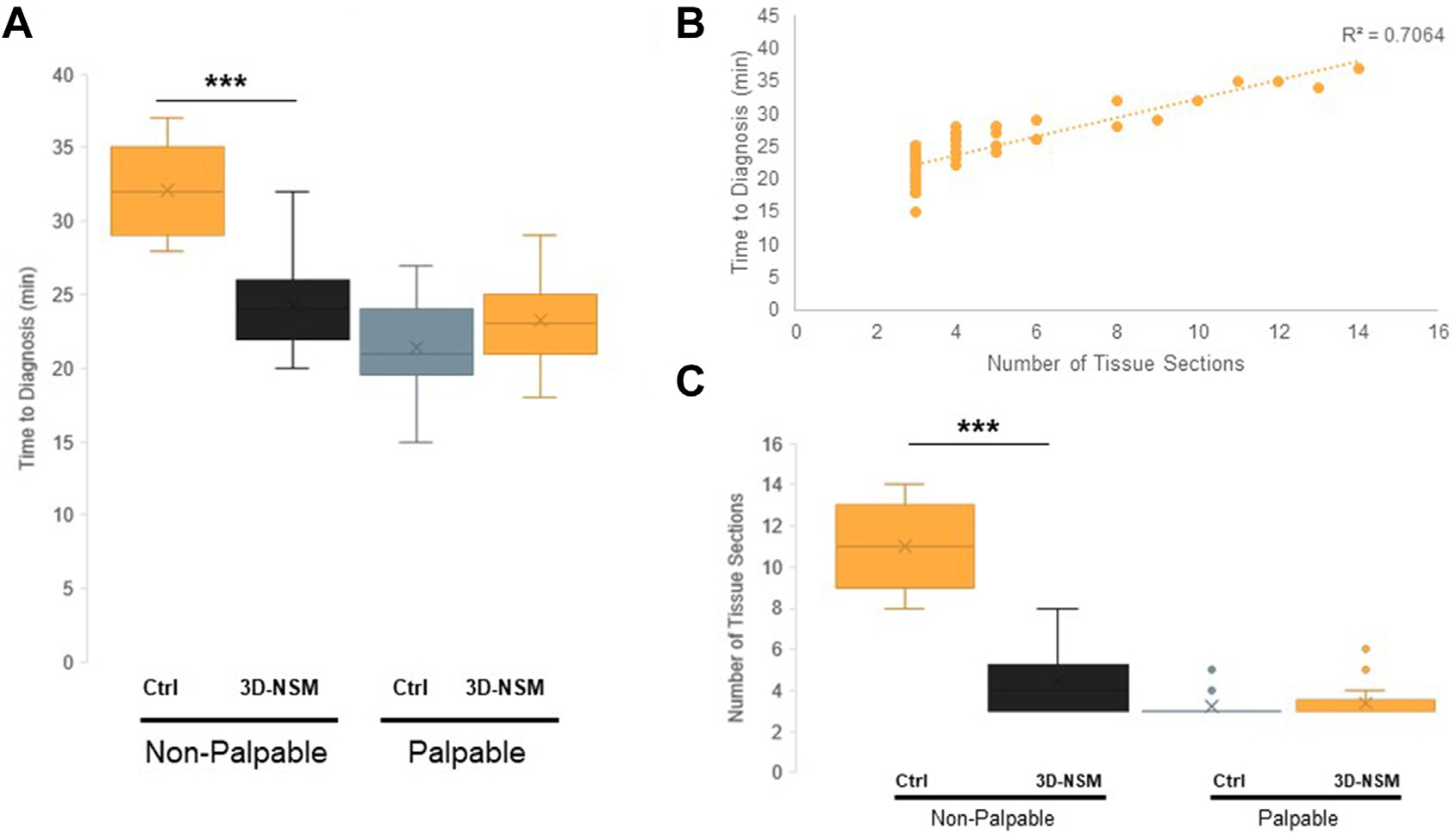
Results: 3D-NSM localized 54 of 55 lesions with 1 false negative. All 41 palpable lesions were identified by 3D-NSM. Thirteen (92.8%) of 14 nonpalpable lesions were located by 3D-NSM. Time to diagnosis for the 3D-NSM cohort was 23.5 minutes, compared with 26.0 minutes in the control cohort (P = .04). 3D-NSM did not affect time to diagnosis of palpable lesions (23.2 minutes vs 21.4 minutes; P = .10). 3D-NSM significantly reduced time to diagnosis for nonpalpable lesions (23.3 minutes vs 34.4 minutes; P < .0001). 3D-NSM also reduced the number of tissue sections analyzed in nonpalpable lesions (4.50 vs 11.00; P < .0001).
Conclusions: 3D-NSM accurately localizes GGOs and expedites intraoperative diagnosis by reducing the number of tissue sections analyzed for nonpalpable GGOs.
Copyright © 2022 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr Low is a shareholder in On Target Laboratories. There are no conflicts of interest for any other author.
Figures
Similar articles
-
Three-Dimensional Near-Infrared Specimen Mapping Can Identify the Distance from the Tumor to the Surgical Margin During Resection of Pulmonary Ground Glass Opacities.Mol Imaging Biol. 2023 Feb;25(1):203-211. doi: 10.1007/s11307-022-01750-0. Epub 2022 Jul 13. Mol Imaging Biol. 2023. PMID: 35831734 Free PMC article.
-
A simple inflation method for frozen section diagnosis of minute precancerous lesions of the lung.Lung Cancer. 2008 Feb;59(2):198-202. doi: 10.1016/j.lungcan.2007.08.023. Epub 2007 Oct 1. Lung Cancer. 2008. PMID: 17905468
-
[Accuracy of intraoperative frozen section diagnosis in non palpable breast lesions: a series of 791 cases].Bull Cancer. 2003 Apr;90(4):357-62. Bull Cancer. 2003. PMID: 12801819 French.
-
[Localized pure or mixed ground-glass lung opacities].J Radiol. 2009 Nov;90(11 Pt 2):1869-92. doi: 10.1016/s0221-0363(09)73289-5. J Radiol. 2009. PMID: 19953078 Review. French.
-
Management of Ground-Glass Opacities in the Lung Cancer Spectrum.Ann Thorac Surg. 2020 Dec;110(6):1796-1804. doi: 10.1016/j.athoracsur.2020.04.094. Epub 2020 Jun 7. Ann Thorac Surg. 2020. PMID: 32525031 Review.
Cited by
-
First-in-human results of targeted intraoperative molecular imaging for visualization of ground glass opacities during robotic pulmonary resection.Transl Lung Cancer Res. 2022 Aug;11(8):1567-1577. doi: 10.21037/tlcr-21-1004. Transl Lung Cancer Res. 2022. PMID: 36090642 Free PMC article.
-
A pH-Activatable Nanoprobe Labels Diverse Histologic Subtypes of Human Lung Cancer During Resection.Mol Imaging Biol. 2023 Oct;25(5):824-832. doi: 10.1007/s11307-023-01853-2. Epub 2023 Sep 11. Mol Imaging Biol. 2023. PMID: 37697109 Free PMC article.
-
Three-Dimensional Near-Infrared Specimen Mapping Can Identify the Distance from the Tumor to the Surgical Margin During Resection of Pulmonary Ground Glass Opacities.Mol Imaging Biol. 2023 Feb;25(1):203-211. doi: 10.1007/s11307-022-01750-0. Epub 2022 Jul 13. Mol Imaging Biol. 2023. PMID: 35831734 Free PMC article.
-
Prospective validation of tumor folate receptor expression density with the association of pafolacianine fluorescence during intraoperative molecular imaging-guided lung cancer resections.Eur J Nucl Med Mol Imaging. 2023 Jul;50(8):2453-2465. doi: 10.1007/s00259-023-06141-3. Epub 2023 Mar 11. Eur J Nucl Med Mol Imaging. 2023. PMID: 36905412 Free PMC article.
-
Single-institution experience of 500 pulmonary resections guided by intraoperative molecular imaging.J Thorac Cardiovasc Surg. 2023 Jun;165(6):1928-1938.e1. doi: 10.1016/j.jtcvs.2022.12.023. Epub 2023 Jan 30. J Thorac Cardiovasc Surg. 2023. PMID: 36863974 Free PMC article.
References
-
- Krist AH, Davidson KW, Mangione CM, et al. Screening for lung cancer: US preventive services task force recommendation statement. JAMA. 2021;325(10):962–970. - PubMed
-
- Pedersen JH, Saghir Z, Wille MMW, Thomsen LH, Skov BG, Ashraf H. Ground-glass opacity lung nodules in the era of lung cancer CT screening: radiology, pathology, and clinical management. Oncology (Williston Park). 2016;30(3):266–274. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
