

Estrogen Inhibits Epithelial Progesterone Receptor-Dependent Progestin Therapy Efficacy in a Mouse Model of Cervical Cancer
- PMID: 34774516
- PMCID: PMC8908498
- DOI: 10.1016/j.ajpath.2021.10.008
Estrogen Inhibits Epithelial Progesterone Receptor-Dependent Progestin Therapy Efficacy in a Mouse Model of Cervical Cancer
Abstract
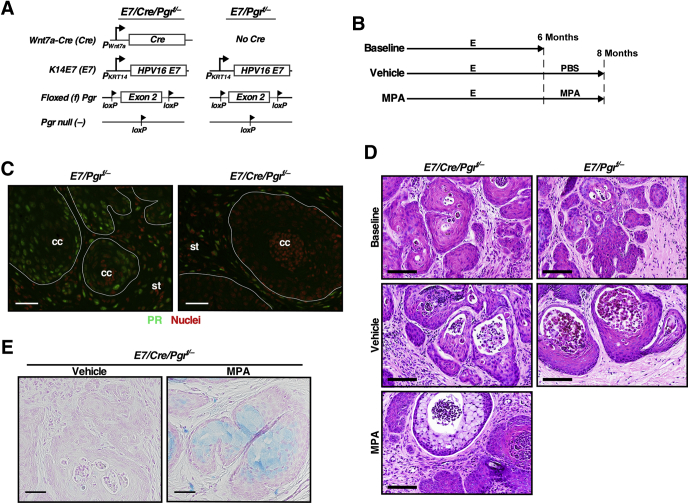
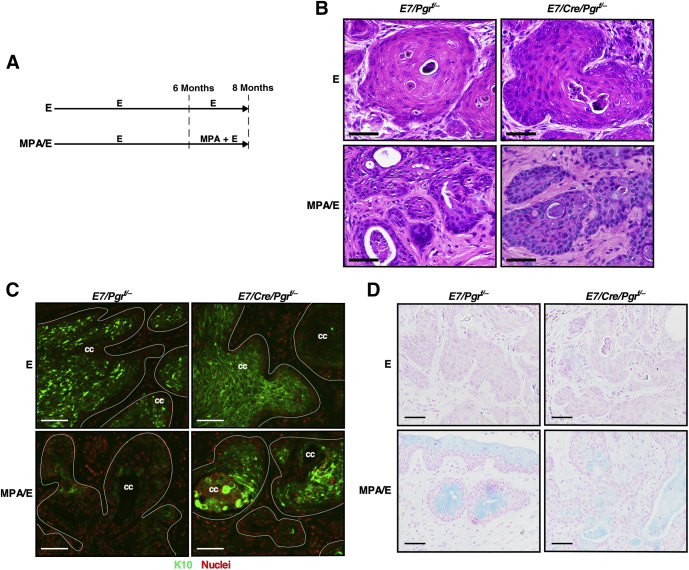
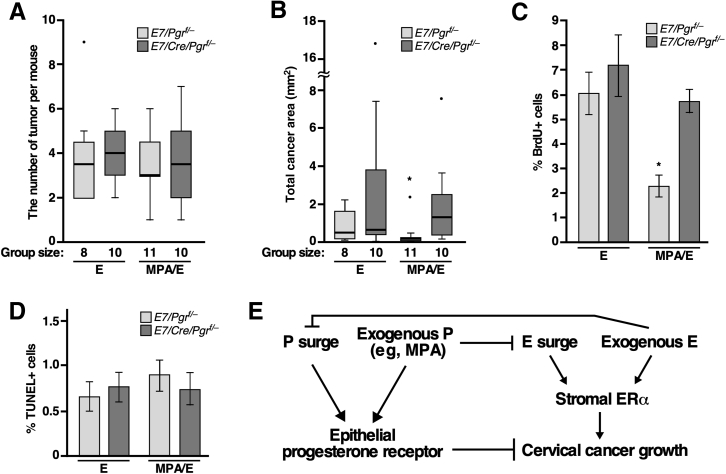
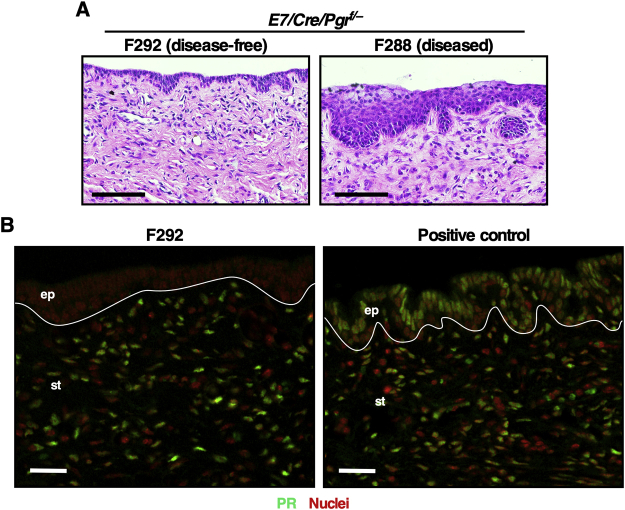
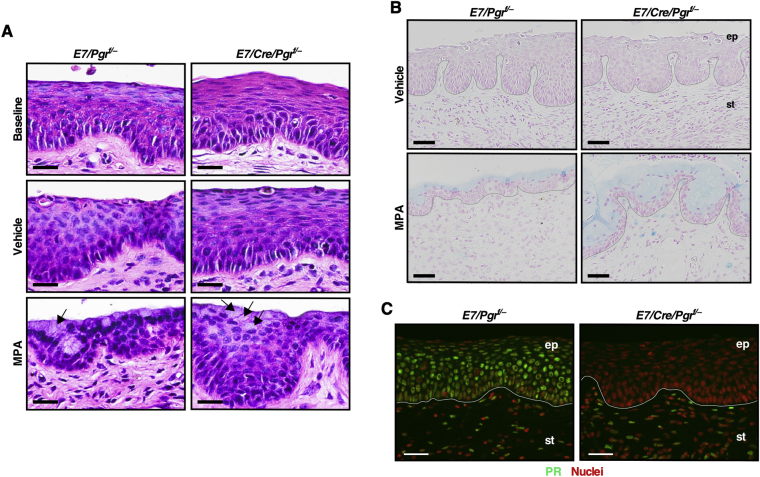
Although the uterine cervix responds to the female sex hormone change, the role of progesterone in cervical cancer is poorly understood. It has been shown that medroxyprogesterone acetate (MPA) regresses cervical cancer in the transgenic mouse model expressing human papillomavirus type 16 E6 and E7 oncogenes. As MPA interacts most strongly with progesterone receptor (PR), we reasoned that PR would contribute to MPA-induced regression of cervical cancer. We also hypothesized that estrogen influences the therapeutic activity of MPA because it promotes cervical cancer growth in the same mouse model. The present study showed that the deletion of Pgr in the cervical cancer cells ablated the MPA's therapeutic effect in the human papillomavirus transgenic mouse model. Additionally, estrogen attenuated cancer regression by MPA in the same model system. These observations indicate that MPA can effectively regress cervical cancer only when cancer cells express PR and estrogen levels are low. These results suggest that, if translatable, MPA should be administered when estrogen levels are low in patients with PR-positive cervical cancer.
Copyright © 2022 American Society for Investigative Pathology. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Progesterone signaling inhibits cervical carcinogenesis in mice.Am J Pathol. 2013 Nov;183(5):1679-1687. doi: 10.1016/j.ajpath.2013.07.026. Epub 2013 Sep 5. Am J Pathol. 2013. PMID: 24012679 Free PMC article.
-
Medroxyprogesterone Acetate Prevention of Cervical Cancer through Progesterone Receptor in a Human Papillomavirus Transgenic Mouse Model.Am J Pathol. 2019 Dec;189(12):2459-2468. doi: 10.1016/j.ajpath.2019.08.013. Epub 2019 Nov 12. Am J Pathol. 2019. PMID: 31732107 Free PMC article.
-
Recurrence of cervical cancer and its resistance to progestin therapy in a mouse model.Oncotarget. 2017 Jan 10;8(2):2372-2380. doi: 10.18632/oncotarget.13676. Oncotarget. 2017. PMID: 27911853 Free PMC article.
-
Role of nuclear progesterone receptor isoforms in uterine pathophysiology.Hum Reprod Update. 2015 Mar-Apr;21(2):155-73. doi: 10.1093/humupd/dmu056. Epub 2014 Nov 18. Hum Reprod Update. 2015. PMID: 25406186 Free PMC article. Review.
-
Reproductive epidemiology of glial tumors may reveal novel treatments: high-dose progestins or progesterone antagonists as endocrino-immune modifiers against glioma.Neurosurg Rev. 2019 Jun;42(2):351-369. doi: 10.1007/s10143-018-0953-1. Epub 2018 Feb 17. Neurosurg Rev. 2019. PMID: 29453736 Review.
Cited by
-
Crosstalk between ferroptosis and steroid hormone signaling in gynecologic cancers.Front Mol Biosci. 2023 Jul 4;10:1223493. doi: 10.3389/fmolb.2023.1223493. eCollection 2023. Front Mol Biosci. 2023. PMID: 37469703 Free PMC article. Review.
-
Effects of perioperative anesthetics on the postoperative prognosis of patients undergoing surgery for cervical cancer.Front Pharmacol. 2025 Mar 10;16:1536663. doi: 10.3389/fphar.2025.1536663. eCollection 2025. Front Pharmacol. 2025. PMID: 40129947 Free PMC article. Review.
-
Astragalus polysaccharide regulates the cervical cancer cell cycle and inhibits cisplatin resistance by blocking the Wnt/β-catenin pathway through the PPARD/CDC20 axis.Cytotechnology. 2025 Aug;77(4):126. doi: 10.1007/s10616-025-00785-9. Epub 2025 Jun 17. Cytotechnology. 2025. PMID: 40538591
-
Risks of Cervical Cancer Recurrence After Fertility-Sparing Surgery and the Role of Human Papillomavirus Infection Types.J Clin Med. 2024 Oct 22;13(21):6318. doi: 10.3390/jcm13216318. J Clin Med. 2024. PMID: 39518458 Free PMC article. Review.
-
Exploring Cervical Adenocarcinoma: Epidemiological Insights, Diagnostic and Therapeutic Challenges, and Pathogenetic Mechanisms.Cancer Med. 2025 Jan;14(2):e70620. doi: 10.1002/cam4.70620. Cancer Med. 2025. PMID: 39840708 Free PMC article. Review.
References
-
- Downs L.S., Smith J.S., Scarinci I., Flowers L., Parham G. The disparity of cervical cancer in diverse populations. Gynecol Oncol. 2008;109:22–30. - PubMed
-
- Larson H.J., Brocard P., Garnett G. The India HPV-vaccine suspension. Lancet. 2010;376:572–573. - PubMed
-
- Ferlay J., Colombet M., Soerjomataram I., Mathers C., Parkin D.M., Pineros M., Znaor A., Bray F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144:1941–1953. - PubMed
