

Interstitial lung disease is a dominant feature in patients with circulating myositis-specific antibodies
- PMID: 34775966
- PMCID: PMC8591876
- DOI: 10.1186/s12890-021-01737-7
Interstitial lung disease is a dominant feature in patients with circulating myositis-specific antibodies
Abstract
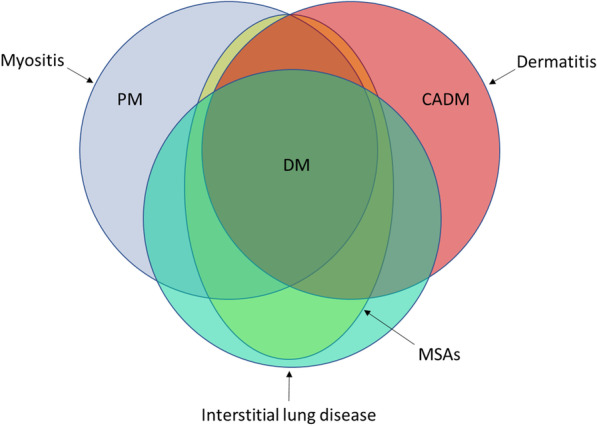
Background: Many patients with polymyositis (PM) or dermatomyositis (DM) have circulating myositis-specific antibodies (MSAs). Interstitial lung disease (ILD) is a common manifestation of PM/DM, and it can even precede the onset of characteristic muscle or skin manifestations. Furthermore, there appear to be some patients with ILD and circulating MSAs who do not develop muscle or skin disease even after prolonged follow-up. We sought to determine whether ILD is equally or more common than myositis or dermatitis at the time of initial detection of MSAs.
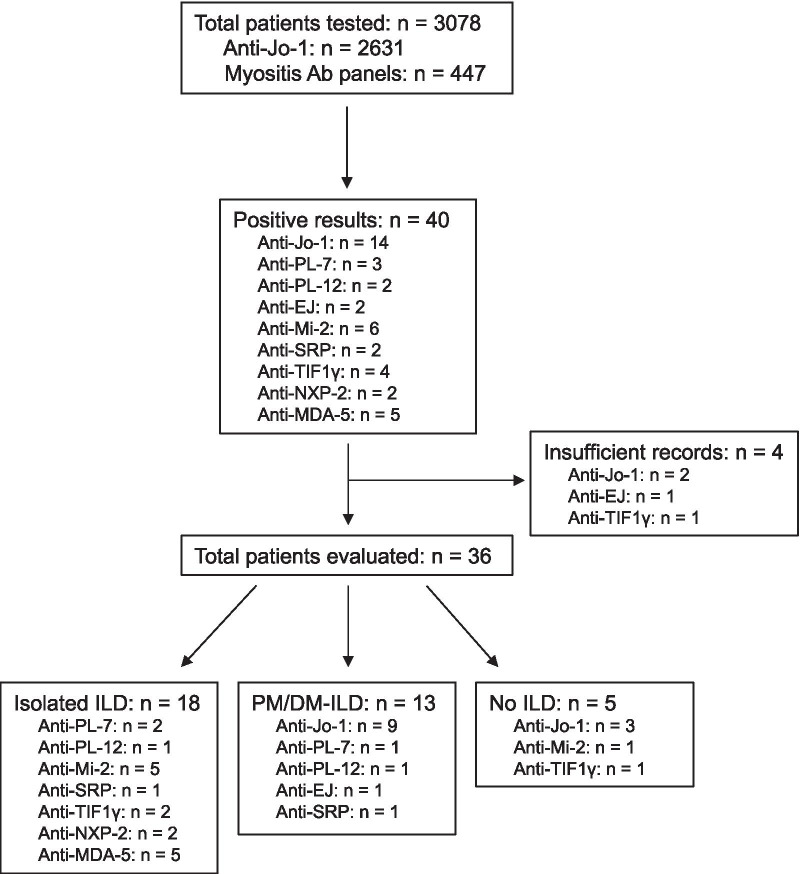
Methods: We identified all patients found to have circulating MSAs at our institution over a 4-year period and assessed for the presence of lung, muscle, and skin disease at the time of initial detection of MSAs. Among those found to have ILD, we compared demographic and clinical features, chest CT scan findings, and outcomes between those with PM/DM-associated ILD and those with ILD but no muscle or skin disease.
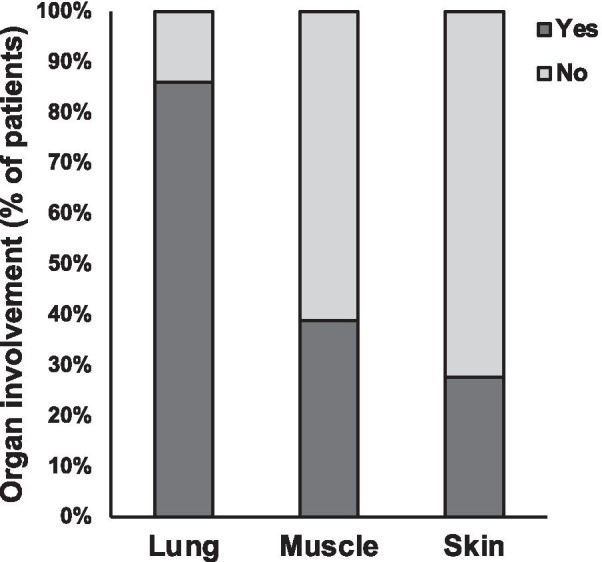
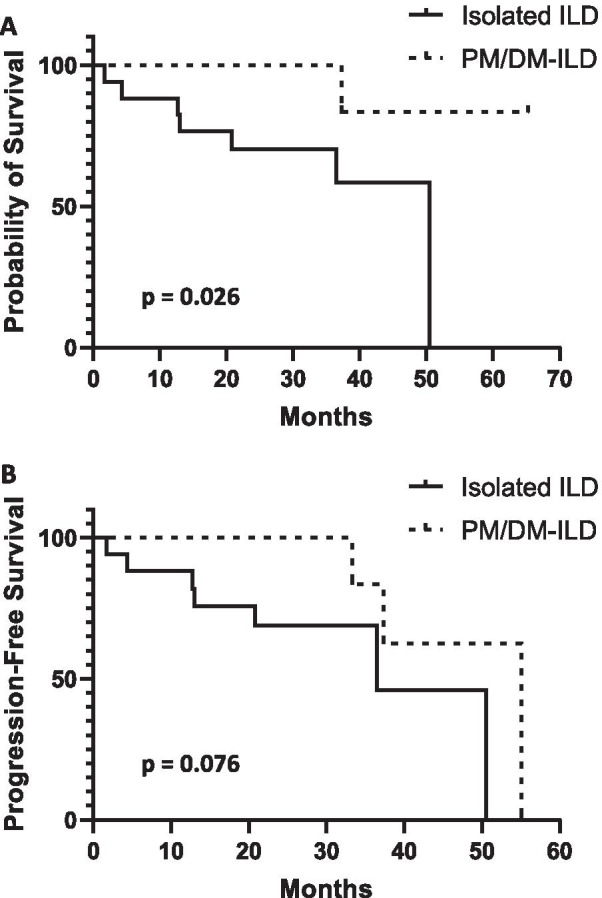
Results: A total of 3078 patients were tested for MSAs, and of these 40 were positive. Nine different MSAs were detected, with anti-histidyl tRNA synthetase (anti-Jo-1) being the most common (35% of MSAs). Among patients with positive MSAs, 86% were found to have ILD, compared to 39% and 28% with muscle and skin involvement, respectively (p < 0.001). Fifty percent of all MSA-positive patients had isolated ILD, with no evidence of muscle or skin disease. Those with isolated ILD were more likely to be older and have fibrotic changes on chest CT, less likely to receive immunomodulatory therapy, and had worse overall survival.
Conclusions: In this study we found that individuals with circulating MSAs were more likely to have ILD than classic muscle or skin manifestations of PM/DM at the time of initial detection of MSAs. Our findings suggest that the presence of ILD should be considered a disease-defining manifestation in the presence of MSAs and incorporated into classification criteria for PM/DM.
Keywords: Dermatomyositis; Interstitial lung disease; Myositis-specific antibodies; Polymyositis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Love LA, Leff RL, Fraser DD, Targoff IN, Dalakas M, Plotz PH, Miller FW. A new approach to the classification of idiopathic inflammatory myopathy: myositis-specific autoantibodies define useful homogeneous patient groups. Medicine (Baltimore) 1991;70:360–374. doi: 10.1097/00005792-199111000-00002. - DOI - PubMed
-
- Hengstman GJ, van Engelen BG, van Venrooij WJ. Myositis specific autoantibodies: changing insights in pathophysiology and clinical associations. Curr Opin Rheumatol. 2004;16:692–699. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
