

Three Technologies That Will Guide Revascularization of Chronic Coronary Syndrome Patients into the 21st Century: A Review
- PMID: 34776821
- PMCID: PMC8580608
- DOI: 10.1055/s-0041-1735201
Three Technologies That Will Guide Revascularization of Chronic Coronary Syndrome Patients into the 21st Century: A Review
Abstract
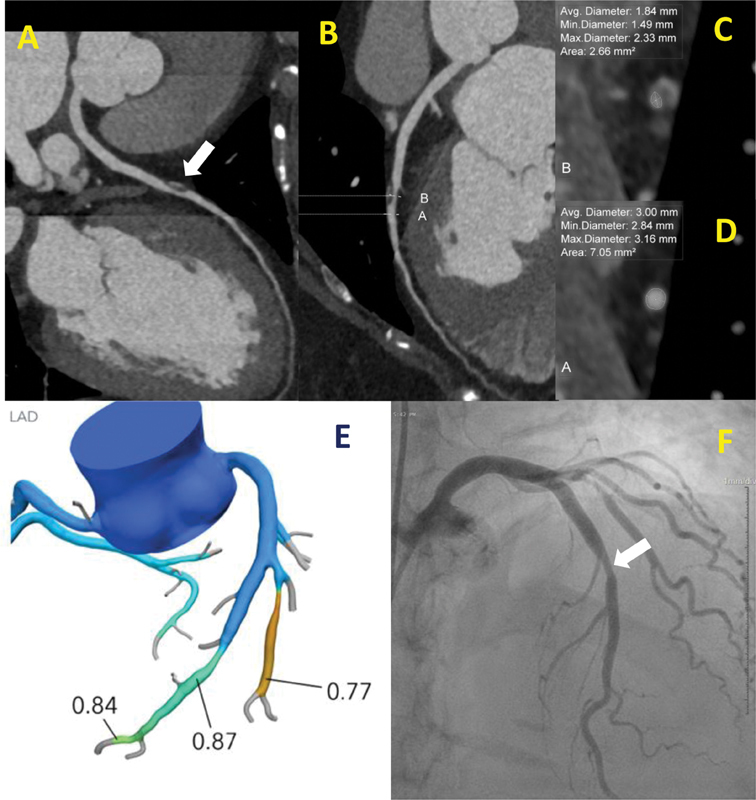
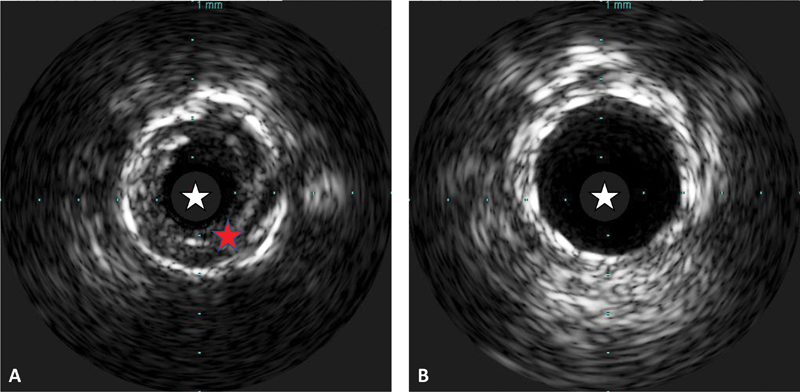
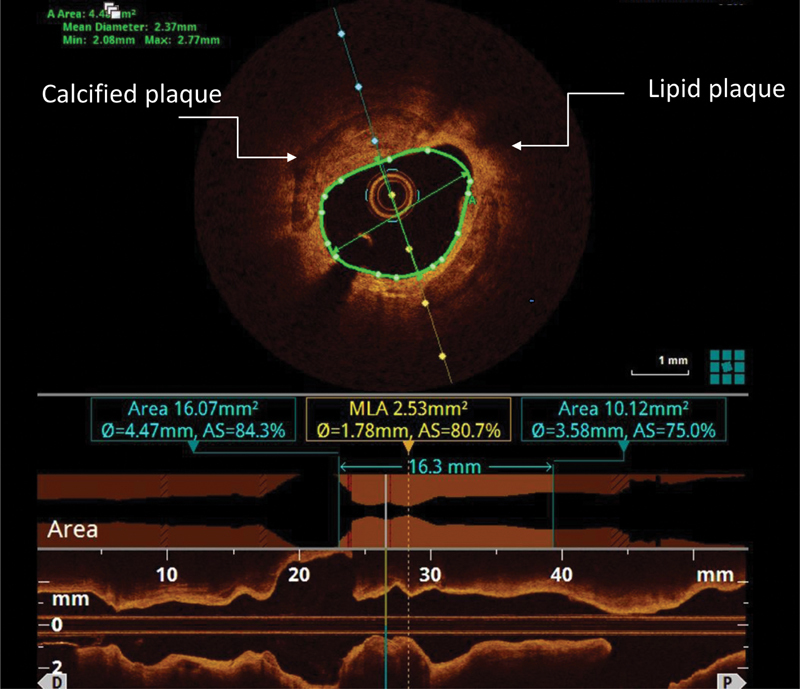
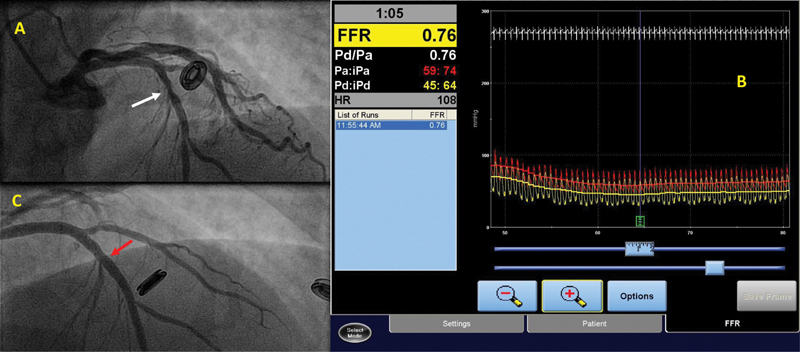
Although medical therapy is the preferred first-line treatment for patients with chronic coronary syndrome (CCS), revascularization remains an important consideration. We present a review that identifies the three diagnostic technologies most important to guiding the decision to revascularize patients with CCS: (1) cardiac computed tomography, (2) intracoronary imaging, and (3) lesion-specific physiological guidance.
Keywords: cardiac computed tomography; chronic coronary syndrome; fractional flow reserve; instantaneous wave-free ratio; intravascular ultrasound; medical therapy; optical coherence tomography; revascularization.
International College of Angiology. This article is published by Thieme.
Conflict of interest statement
Conflict of Interest None declared.
Figures


Similar articles
-
The Role of Fractional Flow Reserve and Instantaneous Wave-Free Ratio Measurements in Patients with Acute Coronary Syndrome.Curr Cardiol Rep. 2019 Nov 25;21(12):159. doi: 10.1007/s11886-019-1233-6. Curr Cardiol Rep. 2019. PMID: 31768835 Review.
-
Intravascular ultrasound or optical coherence tomography-defined anatomic severity and hemodynamic severity assessed by coronary physiologic indices.Rev Esp Cardiol (Engl Ed). 2020 Oct;73(10):812-821. doi: 10.1016/j.rec.2019.11.001. Epub 2019 Dec 4. Rev Esp Cardiol (Engl Ed). 2020. PMID: 31812517 English, Spanish.
-
Usefulness of coronary fractional flow reserve measurements in guiding clinical decisions in intermediate or equivocal left main coronary stenoses.Am J Cardiol. 2009 Apr 1;103(7):943-9. doi: 10.1016/j.amjcard.2008.11.054. Epub 2009 Feb 7. Am J Cardiol. 2009. PMID: 19327420
-
Diagnostic accuracy of a hybrid approach of instantaneous wave-free ratio and fractional flow reserve using high-dose intracoronary adenosine to characterize intermediate coronary lesions: Results of the PALS (Practical Assessment of Lesion Severity) prospective study.Catheter Cardiovasc Interv. 2017 Dec 1;90(7):1070-1076. doi: 10.1002/ccd.27038. Epub 2017 May 22. Catheter Cardiovasc Interv. 2017. PMID: 28544741
-
The Impact of Coronary Physiology on Contemporary Clinical Decision Making.JACC Cardiovasc Interv. 2020 Jul 27;13(14):1617-1638. doi: 10.1016/j.jcin.2020.04.040. JACC Cardiovasc Interv. 2020. PMID: 32703589 Review.
References
-
- The top Ten Causes of Death. World Health Organization Website https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death. Updated 9 December 2020, Accessed July 29, 2021
-
- Agostoni P, Biondi-Zoccai G G, Gasparini G L. Is bare-metal stenting superior to balloon angioplasty for small vessel coronary artery disease? Evidence from a meta-analysis of randomized trials. Eur Heart J. 2005;26(09):881–889. - PubMed
-
- Sabaté M, Brugaletta S, Cequier A.Clinical outcomes in patients with ST-segment elevation myocardial infarction treated with everolimus-eluting stents versus bare-metal stents (EXAMINATION): 5-year results of a randomised trial Lancet 2016387(10016):357–366. - PubMed
