

Representation of Body Orientation in Vestibular-Defective Patients Before and After Unilateral Vestibular Loss
- PMID: 34776883
- PMCID: PMC8580062
- DOI: 10.3389/fnsys.2021.733684
Representation of Body Orientation in Vestibular-Defective Patients Before and After Unilateral Vestibular Loss
Abstract
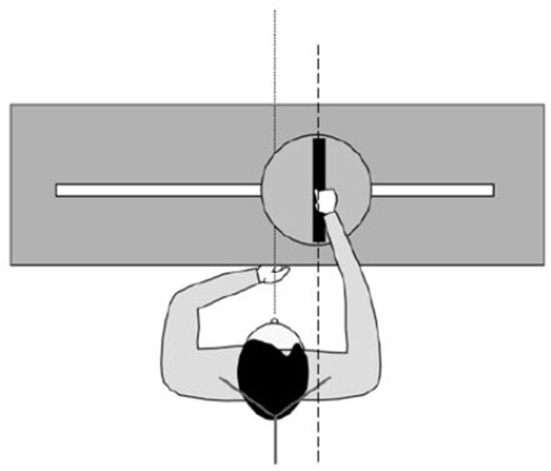
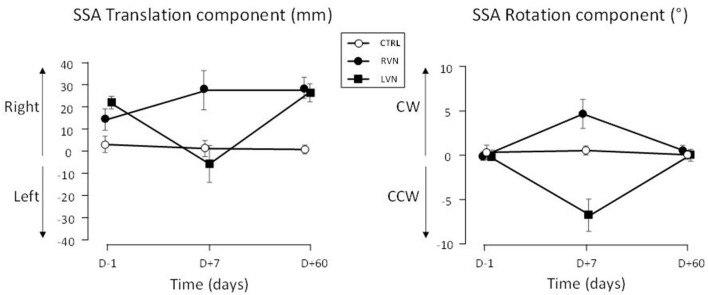
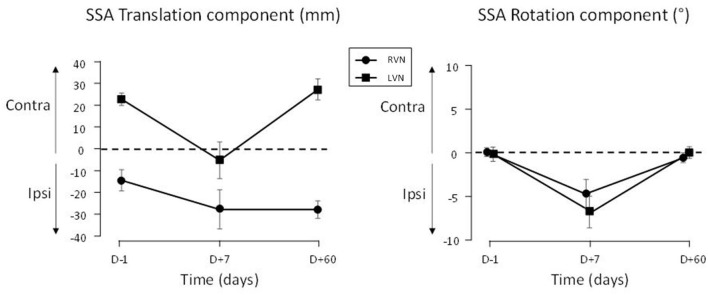
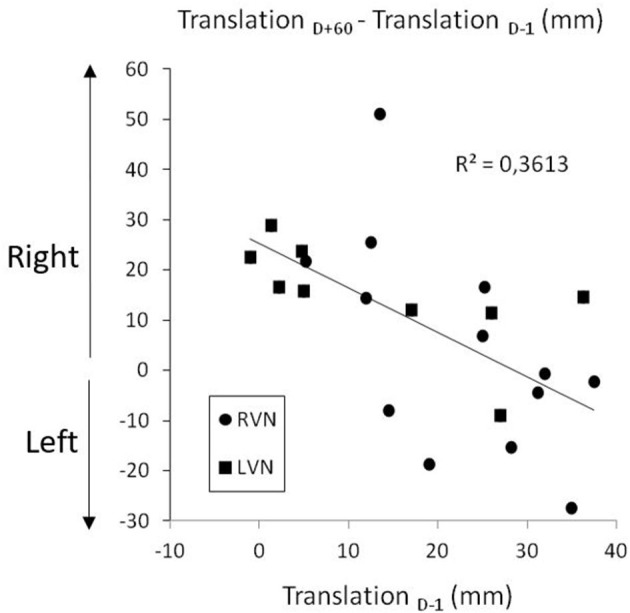
Introduction: The unilateral vestibular syndrome results in postural, oculomotor, perceptive, and cognitive symptoms. This study was designed to investigate the role of vestibular signals in body orientation representation, which remains poorly considered in vestibular patients. Methods: The subjective straight ahead (SSA) was investigated using a method disentangling translation and rotation components of error. Participants were required to align a rod with their body midline in the horizontal plane. Patients with right vestibular neurotomy (RVN; n =8) or left vestibular neurotomy (LVN; n = 13) or vestibular schwannoma resection were compared with 12 healthy controls. Patients were tested the day before surgery and during the recovery period, 7 days and 2 months after the surgery. Results: Before and after unilateral vestibular neurotomy, i.e., in the chronic phases, patients showed a rightward translation bias of their SSA, without rotation bias, whatever the side of the vestibular loss. However, the data show that the lower the translation error before neurotomy, the greater its increase 2 months after a total unilateral vestibular loss, therefore leading to a rightward translation of similar amplitude in the two groups of patients. In the early phase after surgery, SSA moved toward the operated side both in translation and in rotation, as typically found for biases occurring after unilateral vestibular loss, such as the subjective visual vertical (SVV) bias. Discussion and Conclusion: This study gives the first description of the immediate consequences and of the recovery time course of body orientation representation after a complete unilateral vestibular loss. The overall evolution differed according to the side of the lesion with more extensive changes over time before and after left vestibular loss. It is noteworthy that representational disturbances of self-orientation were highly unusual in the chronic stage after vestibular loss and similar to those reported after hemispheric lesions causing spatial neglect, while classical ipsilesional biases were reported in the acute stage. This study strongly supports the notion that the vestibular system plays a major role in body representation processes and more broadly in spatial cognition. From a clinical point of view, SSA appeared to be a reliable indicator for the presence of a vestibular disorder.
Keywords: recovery time-course; spatial cognition; spatial orientation; subjective visual straight ahead; unilateral vestibular loss.
Copyright © 2021 Borel, Honoré, Bachelard-Serra, Lavieille and Saj.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Where is straight ahead to a patient with unilateral vestibular loss?Cortex. 2013 May;49(5):1219-28. doi: 10.1016/j.cortex.2012.05.019. Epub 2012 Jun 18. Cortex. 2013. PMID: 22795184
-
Signs of spatial neglect in unilateral peripheral vestibulopathy.Eur J Neurol. 2021 May;28(5):1779-1783. doi: 10.1111/ene.14701. Epub 2021 Jan 19. Eur J Neurol. 2021. PMID: 33369817
-
Reducing rightward bias of subjective straight ahead in neglect patients by changes in body orientation.J Neurol Neurosurg Psychiatry. 2008 Sep;79(9):991-6. doi: 10.1136/jnnp.2007.124412. Epub 2008 Jan 25. J Neurol Neurosurg Psychiatry. 2008. PMID: 18223012
-
Perception of Verticality and Vestibular Disorders of Balance and Falls.Front Neurol. 2019 Apr 3;10:172. doi: 10.3389/fneur.2019.00172. eCollection 2019. Front Neurol. 2019. PMID: 31001184 Free PMC article. Review.
-
Vestibular syndrome: a change in internal spatial representation.Neurophysiol Clin. 2008 Dec;38(6):375-89. doi: 10.1016/j.neucli.2008.09.002. Epub 2008 Oct 7. Neurophysiol Clin. 2008. PMID: 19026958 Review.
Cited by
-
Recent developments in the understanding of the interactions between the vestibular system, memory, the hippocampus, and the striatum.Front Neurol. 2022 Sep 2;13:986302. doi: 10.3389/fneur.2022.986302. eCollection 2022. Front Neurol. 2022. PMID: 36119673 Free PMC article. Review.
-
Innovative approaches for managing patients with chronic vestibular disorders: follow-up indicators and predictive markers for studying the vestibular error signal.Front Rehabil Sci. 2024 Aug 16;5:1414198. doi: 10.3389/fresc.2024.1414198. eCollection 2024. Front Rehabil Sci. 2024. PMID: 39220608 Free PMC article.
-
Vestibular perceptual testing from lab to clinic: a review.Front Neurol. 2023 Oct 4;14:1265889. doi: 10.3389/fneur.2023.1265889. eCollection 2023. Front Neurol. 2023. PMID: 37859653 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials