

Sex Differences in Cerebral Small Vessel Disease: A Systematic Review and Meta-Analysis
- PMID: 34777227
- PMCID: PMC8581736
- DOI: 10.3389/fneur.2021.756887
Sex Differences in Cerebral Small Vessel Disease: A Systematic Review and Meta-Analysis
Abstract
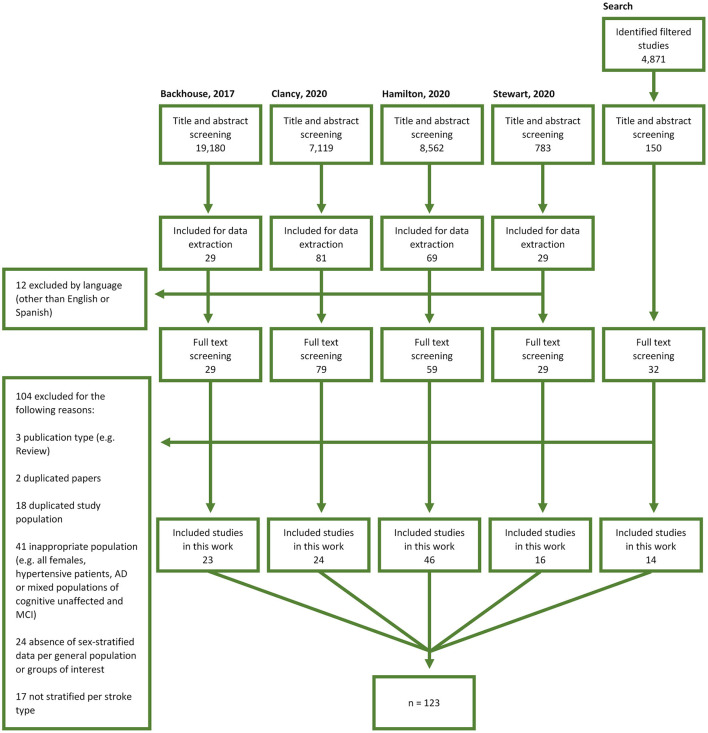
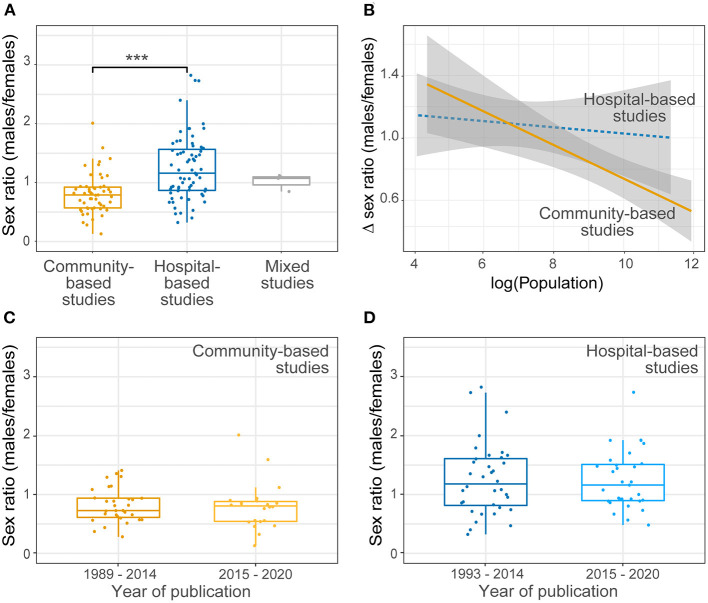
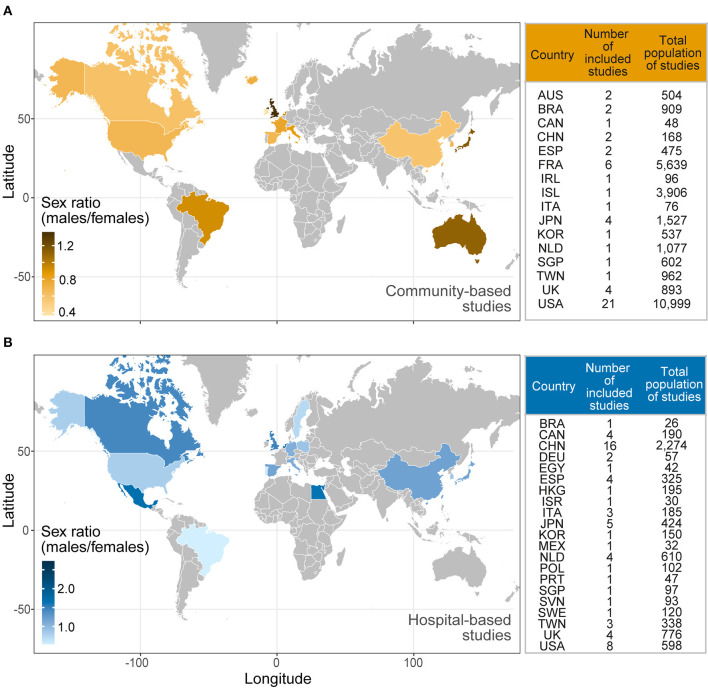
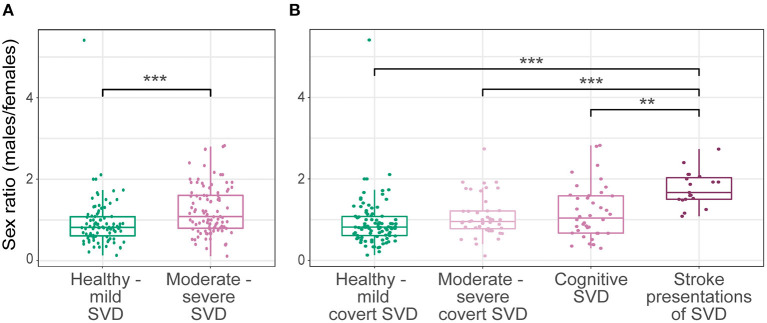
Background: Cerebral small vessel disease (SVD) is a common cause of stroke, mild cognitive impairment, dementia and physical impairments. Differences in SVD incidence or severity between males and females are unknown. We assessed sex differences in SVD by assessing the male-to-female ratio (M:F) of recruited participants and incidence of SVD, risk factor presence, distribution, and severity of SVD features. Methods: We assessed four recent systematic reviews on SVD and performed a supplementary search of MEDLINE to identify studies reporting M:F ratio in covert, stroke, or cognitive SVD presentations (registered protocol: CRD42020193995). We meta-analyzed differences in sex ratios across time, countries, SVD severity and presentations, age and risk factors for SVD. Results: Amongst 123 relevant studies (n = 36,910 participants) including 53 community-based, 67 hospital-based and three mixed studies published between 1989 and 2020, more males were recruited in hospital-based than in community-based studies [M:F = 1.16 (0.70) vs. M:F = 0.79 (0.35), respectively; p < 0.001]. More males had moderate to severe SVD [M:F = 1.08 (0.81) vs. M:F = 0.82 (0.47) in healthy to mild SVD; p < 0.001], and stroke presentations where M:F was 1.67 (0.53). M:F did not differ for recent (2015-2020) vs. pre-2015 publications, by geographical region, or age. There were insufficient sex-stratified data to explore M:F and risk factors for SVD. Conclusions: Our results highlight differences in male-to-female ratios in SVD severity and amongst those presenting with stroke that have important clinical and translational implications. Future SVD research should report participant demographics, risk factors and outcomes separately for males and females. Systematic Review Registration: [PROSPERO], identifier [CRD42020193995].
Keywords: cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL); cerebral small vessel disease (SVD); lacunar stroke; sex differences; vascular dementia (VaD).
Copyright © 2021 Jiménez-Sánchez, Hamilton, Clancy, Backhouse, Stewart, Stringer, Doubal and Wardlaw.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer CC declared a past co-authorship with one of the authors JMW to the handling editor.
Figures
References
-
- Gao Z, Chen Z, Sun A, Deng X. Gender differences in cardiovascular disease. Med Novel Technol Dev. (2019) 4:100025. 10.1016/j.medntd.2019.100025 - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources