

Haploidentical Stem Cell Transplantation for Acute Myeloid Leukemia: Current Therapies, Challenges and Future Prospective
- PMID: 34778077
- PMCID: PMC8581046
- DOI: 10.3389/fonc.2021.758512
Haploidentical Stem Cell Transplantation for Acute Myeloid Leukemia: Current Therapies, Challenges and Future Prospective
Abstract
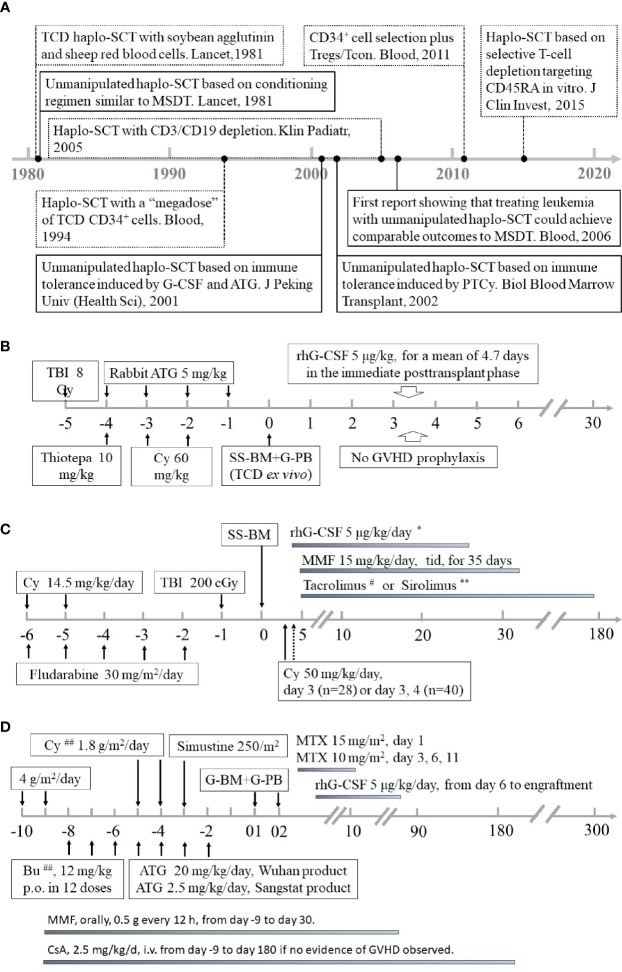
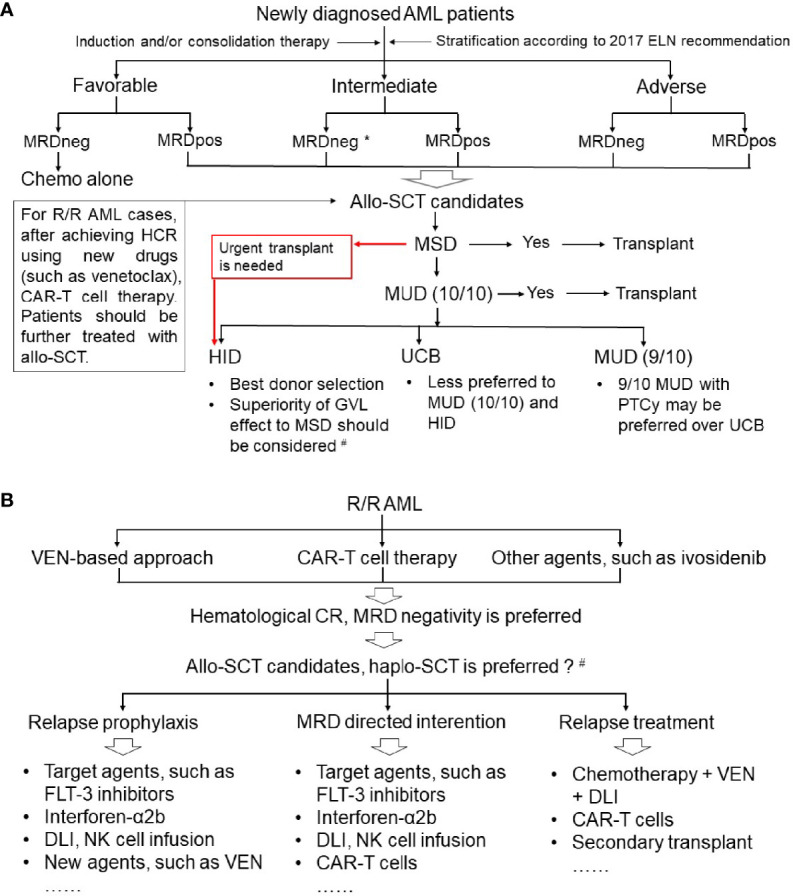
Haploidentical stem cell transplantation (haplo-SCT), an alternative donor source, offers a curative therapy for patients with acute myeloid leukemia (AML) who are transplant candidates. Advances in transplantation techniques, such as donor selection, conditioning regimen modification, and graft-versus-host disease prophylaxis, have successfully improved the outcomes of AML patients receiving haplo-SCT and extended the haploidentical transplant indictions for AML. Presently, treating de novo AML, secondary AML, therapy-related AML and refractory and relapsed AML with haplo-SCT can achieve comparable outcomes to those of human leukocyte antigen (HLA)-matched sibling donor transplantation (MSDT), unrelated donor transplantation or umbilical cord blood transplantation. For some subgroups of AML subjects, such as patients with positive pretransplantation minimal/measurable residual disease, recent studies suggest that haplo-SCT might be superior to MSDT in decreasing relapse and improving survival. Unfortunately, for patients with AML after haplo-SCT, relapse and infections remain the causes of death that restrict further improvement in clinical outcomes. In this review, we discuss the recent advances and challenges in haplo-SCT for AML treatment, mainly focusing on unmanipulated haplo-SCT protocols. We provide an outlook on future prospects and suggest that relapse prophylaxis, intervention, and treatment, as well as infection prevention and therapy, are areas of active research in AML patients who receive haploidentical allografts.
Keywords: acute myeloid leukemia; graft-versus-leukemia-effect; haploidentical stem cell transplantation; infection; relapse.
Copyright © 2021 Chang, Zhao and Huang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Huang XJ, Zhu HH, Chang YJ, Xu LP, Liu DH, Zhang XH, et al. The Superiority of Haploidentical Related Stem Cell Transplantation Over Chemotherapy Alone as Postremission Treatment for Patients With Intermediate- or High-Risk Acute Myeloid Leukemia in First Complete Remission. Blood (2012) 119:5584–90. doi: 10.1182/blood-2011-11-389809 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials