

Recognizing a MIS-Chievous Cause of Acute Viral Gastroenteritis
- PMID: 34778138
- PMCID: PMC8588082
- DOI: 10.3389/fped.2021.748368
Recognizing a MIS-Chievous Cause of Acute Viral Gastroenteritis
Abstract
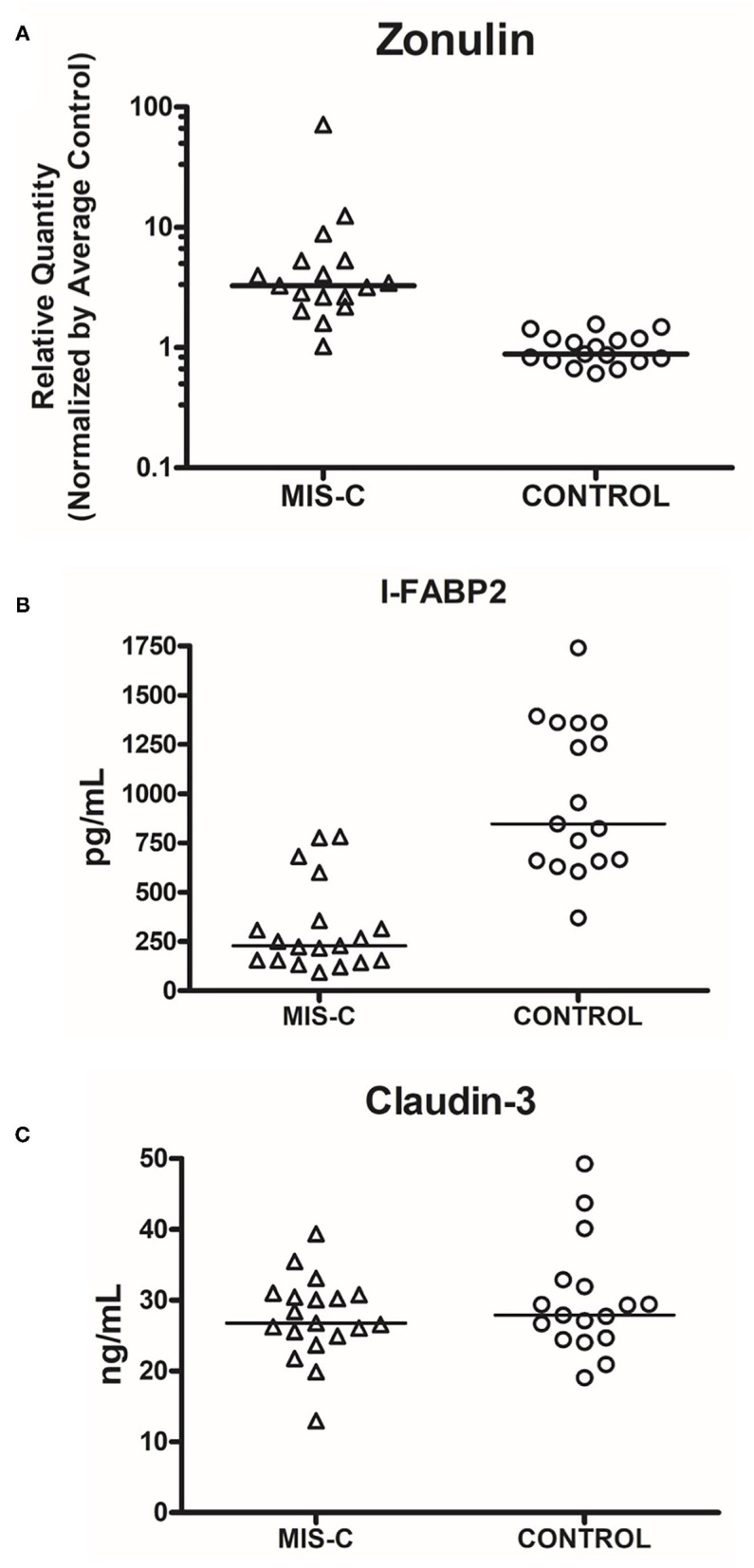
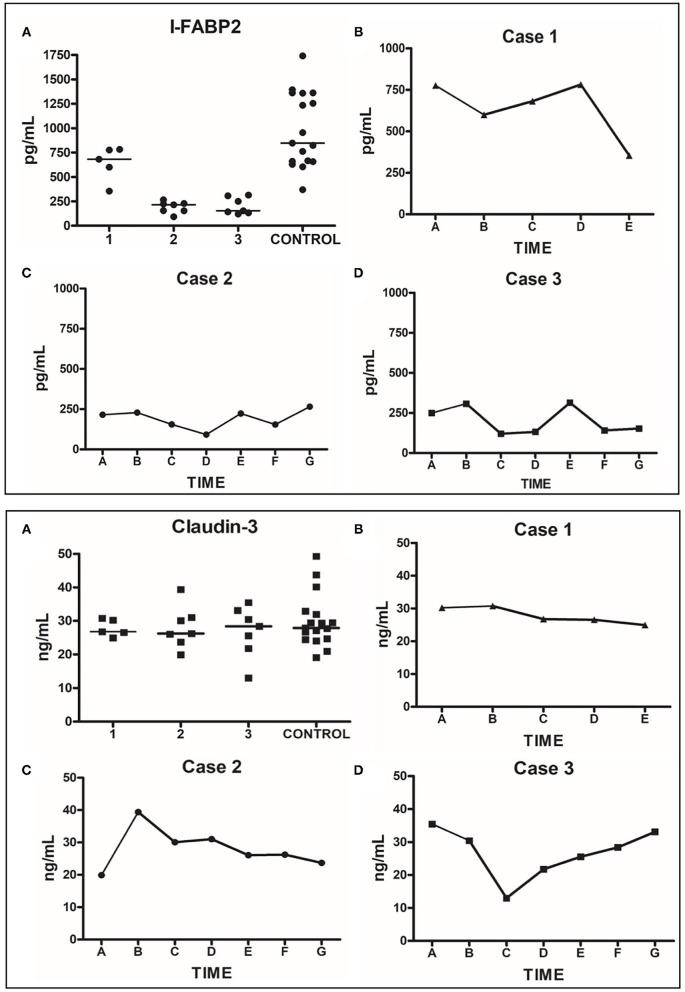
Historically, children evaluated for vomiting and diarrhea secondary to viral enteritis have symptoms lasting 2-4 days and respond to supportive care, including oral rehydration and anti-emetics if required. Recently, within a 14-day timespan, we encountered three children with severe diarrhea who rapidly became dehydrated and went into hypotensive shock. Although SARS-CoV-2 molecular tests were negative by nasopharyngeal swab, all were later found to have MIS-C. This small case series underscores features reported in previous larger studies and emphasizes the rapid clinical evolution of this condition. We highlight the importance of early recognition of cardinal laboratory findings characteristic of MIS-C (i.e., lymphopenia, markedly elevated acute phase reactants, and hypoalbuminemia). We also show serologic evidence that the pathophysiological mechanism of SARS-CoV-2 related diarrhea may differ from other causes of dehydrating vomiting and diarrhea, with no serologic evidence of villus cell injury.
Keywords: I-FABP2; MIS-C multisystem inflammatory syndrome in children; claudin-3; diarrhea; zonulin.
Copyright © 2021 Josyabhatla, Kamdar, Armbrister, Daniel, Boukas, Smith, Van Arsdall, Kakarala, Flores, Wanger, Liu and Rhoads.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Feldstein LR, Tenforde MW, Friedman KG, Newhams M, Rose EB, Dapul H, et al. . Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA. (2021) 325:1074–87. 10.1001/jama.2021.2091 - DOI - PMC - PubMed
-
- The CDC Health Alert Network . Multisystem Inflammatory Syndrome in Children (MIS-C) Associated With Coronavirus Disease 2019 (COVID-19). Centers for Disease Control and Prevention Emergency Preparedness and Response; (2020).
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous