

Pediatric Simplified Acute Physiology Score II: Establishment of a New, Repeatable Pediatric Mortality Risk Assessment Score
- PMID: 34778148
- PMCID: PMC8583491
- DOI: 10.3389/fped.2021.757822
Pediatric Simplified Acute Physiology Score II: Establishment of a New, Repeatable Pediatric Mortality Risk Assessment Score
Abstract
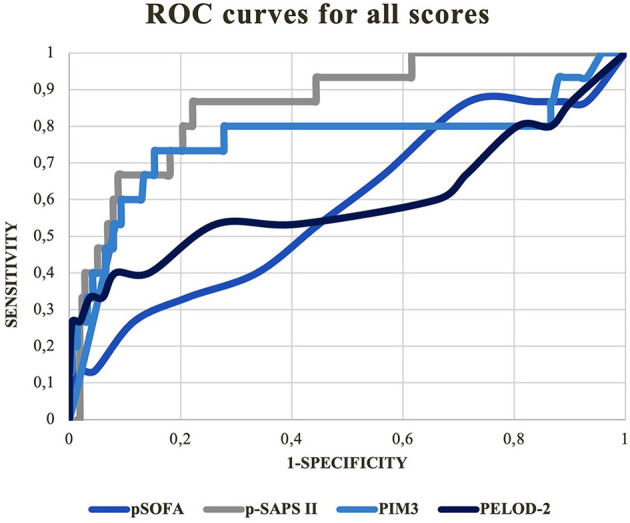
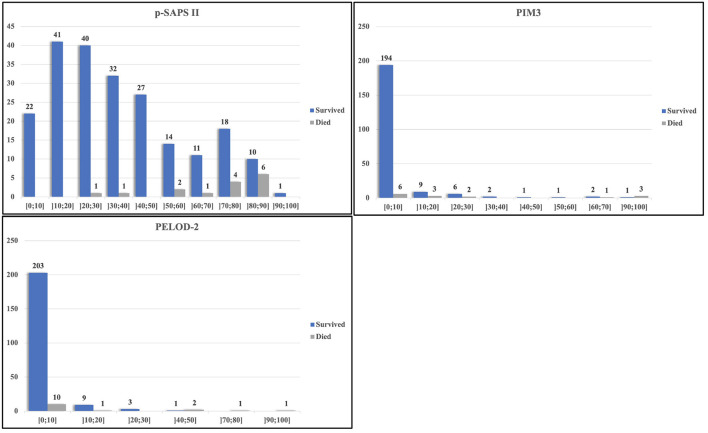
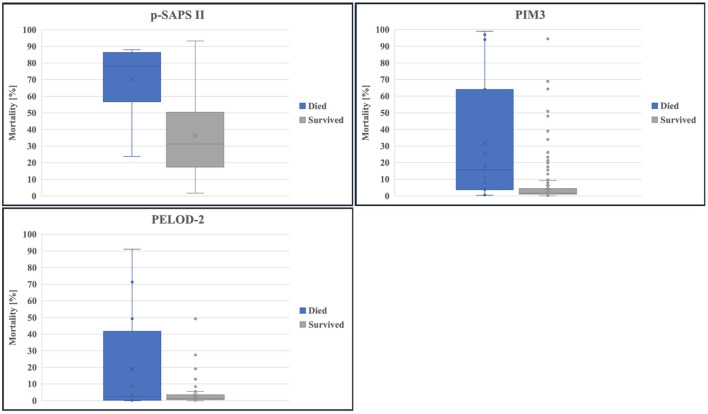
Objectives: In critical care it is crucial to appropriately assess the risk of mortality for each patient. This is especially relevant in pediatrics, with its need for accurate and repeatable scoring. Aim of this study was to evaluate an age-adapted version of the expanded Simplified Acute Physiology Score II; (p-SAPS II), a repeatable, newly-designed scoring system compared to established scores (Pediatric Sequential Organ Failure Assessment Score/pSOFA, Pediatric Logistic Organ Dysfunction Score-2/PELOD-2 and Pediatric Index of Mortality 3/PIM3). Design: This retrospective cohort pilot study included data collected from patients admitted to the Pediatric Intensive Care Unit (PICU) at the Medical University of Vienna between July 2017 through December 2018. Patients: 231 admissions were included, comprising neonates (gestational age of ≥ 37 weeks) and patients up to 18 years of age with a PICU stay longer than 48 h. Main Outcomes: Mortality risk prediction and discrimination between survivors and non-survivors were the main outcomes of this study. The primary statistical methods for evaluating the performance of each score were the area under the receiver operating characteristic curve (AUROC) and goodness-of-fit test. Results: Highest AUROC curve was calculated for p-SAPS II (AUC = 0.86; 95% CI: 0.77-0.96; p < 0.001). This was significantly higher than the AUROCs of PELOD-2/pSOFA but not of PIM3. However, in a logistic regression model including p-SAPS II and PIM3 as covariates, p-SAPS II had a significant effect on the accuracy of prediction (p = 0.003). Nevertheless, according to the goodness-of-fit test for p-SAPS II and PIM3, p-SAPS II overestimated the number of deaths, whereas PIM3 showed acceptable estimations. Repeatability testing showed increasing AUROC values for p-SAPS II throughout the clinical stay (0.96 at day 28) but still no significant difference to PIM 3. The prediction accuracy, although improved over the days and even exceeded PIM 3. Conclusions: The newly-created p-SAPS II performed better than the established PIM3 in terms of discriminating between survivors and non-survivors. Furthermore, p-SAPS II can be assessed repeatably throughout a patient's PICU stay what improves mortality prediction. However, there is still a need to optimize calibration of the score to accurately predict mortality sooner throughout the clinical stay.
Keywords: critical care; mortality; pediatrics–children; risk assessment; scoring systems.
Copyright © 2021 Irschik, Veljkovic, Golej, Schlager, Brandt, Krall and Hermon.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Performance of Sequential Organ Failure Assessment and Simplified Acute Physiology Score II for Post-Cardiac Surgery Patients in Intensive Care Unit.Front Cardiovasc Med. 2021 Dec 6;8:774935. doi: 10.3389/fcvm.2021.774935. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34938790 Free PMC article.
-
The Various Scoring Systems in Pediatric Intensive Care Units: A Prospective Observational Study.Cureus. 2023 May 30;15(5):e39679. doi: 10.7759/cureus.39679. eCollection 2023 May. Cureus. 2023. PMID: 37398718 Free PMC article.
-
Predictive Performance of the Simplified Acute Physiology Score (SAPS) II and the Initial Sequential Organ Failure Assessment (SOFA) Score in Acutely Ill Intensive Care Patients: Post-Hoc Analyses of the SUP-ICU Inception Cohort Study.PLoS One. 2016 Dec 22;11(12):e0168948. doi: 10.1371/journal.pone.0168948. eCollection 2016. PLoS One. 2016. PMID: 28006826 Free PMC article.
-
The Simplified Acute Physiology Score III Is Superior to the Simplified Acute Physiology Score II and Acute Physiology and Chronic Health Evaluation II in Predicting Surgical and ICU Mortality in the "Oldest Old".Curr Gerontol Geriatr Res. 2014;2014:934852. doi: 10.1155/2014/934852. Epub 2014 Feb 17. Curr Gerontol Geriatr Res. 2014. PMID: 24696680 Free PMC article. Review.
-
Severity of illness and organ dysfunction scoring systems in pediatric critical care: The impacts on clinician's practices and the future.Front Pediatr. 2022 Nov 22;10:1054452. doi: 10.3389/fped.2022.1054452. eCollection 2022. Front Pediatr. 2022. PMID: 36483470 Free PMC article. Review.
Cited by
-
Copeptin Release in Arterial Hypotension and Its Association with Severity of Disease in Critically Ill Children.Children (Basel). 2022 May 28;9(6):794. doi: 10.3390/children9060794. Children (Basel). 2022. PMID: 35740731 Free PMC article.
References
LinkOut - more resources
Full Text Sources