

Early Efficacy of Type I Collagen-Based Matrix-Assisted Autologous Chondrocyte Transplantation for the Treatment of Articular Cartilage Lesions
- PMID: 34778233
- PMCID: PMC8584836
- DOI: 10.3389/fbioe.2021.760179
Early Efficacy of Type I Collagen-Based Matrix-Assisted Autologous Chondrocyte Transplantation for the Treatment of Articular Cartilage Lesions
Abstract
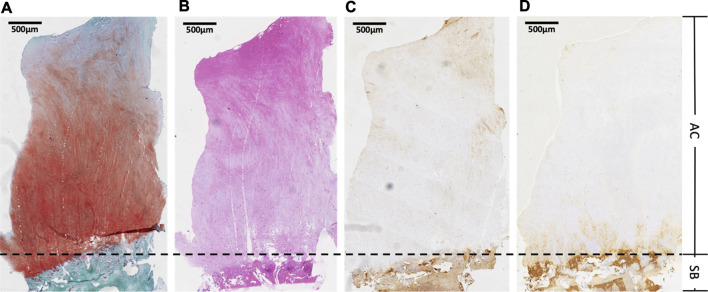
Background: Articular cartilage is a complex structure that allows for low frictional gliding and effective shock absorption. Various sports injuries and inflammatory conditions can lead to lesions in the articular cartilage, which has limited regenerative potential. Type I collagen combined with autologous chondrocytes in a three-dimensional culture were used to induce the regeneration of single-layer autologous expanded chondrocytes without chondrogenic differentiation. Purpose: To assess the clinical, radiological, and histological changes following collagen-based autologous chondrocyte transplantation (MACT) for chondral knee lesions. Methods: The study prospectively enrolled 20 patients with symptomatic knee chondral lesions (mean size lesion was 2.41 ± 0.43 cm2, range: 2.0-3.4 cm2) in the lateral femoral condyle and femoral groove who underwent type I collagen-based MACT between July 2017 and July 2019. knee injury and osteoarthritis outcome score (KOOS) was assessed before the procedure, and periodic clinical follow-up was conducted every 3 months for a maximum of 12 months following the procedure and at 1-year intervals thereafter. Magnetic resonance imaging (MRI) T2 mapping of repaired cartilage was also used for the quantitative analysis of regeneration. In one patient, second-look arthroscopy was performed to assess cartilage regeneration characteristics, and a portion of regenerated cartilage was harvested for histological evaluation 12 months after implantation. Results: At pre-operation and at three, six, 12, and 24 months after the operation, KOOS pain, symptoms, daily life activities, sports and recreation, as well as the quality of life were significantly improved between every two time points. Hematoxylin and eosin (HE) staining indicated that the newly formed cartilage was comprised of naive chondrocytes. Safranin O-fast (S-O) green staining of the regenerated tissue revealed fibroblast-like cells surrounded by glycosaminoglycans. Immunohistochemistry (IHC) analysis indicated that collagen type II was uniformly distributed at the deep zone of articular cartilage and type I collagen mainly depositing in the superficial cartilage layer. The T2 values for repaired tissue gradually decreased, eventually approaching near-average values. Conclusion: The present study demonstrated that type I collagen-based MACT is a clinically effective treatment for improving functionality and pain levels. Histological evidence confirmed hyaline cartilage induction and showed that repaired cartilage tended to emerge from the deep to the superficial layer. The quantitative MRI T2 mapping test indicated that there still was a difference between the transplanted cartilage and the surrounding hyaline cartilage. Taken together, the current method represents an efficient approach for the restoration of knee cartilage lesions.
Keywords: articular cartilage; autologous chondrocyte transplantation; collagen; hyaline; lesion.
Copyright © 2021 Li, Li, Qian, Chen, Zhou and Fu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
-
- Barié A., Kruck P., Sorbi R., Rehnitz C., Oberle D., Walker T., et al. (2020). Prospective Long-Term Follow-Up of Autologous Chondrocyte Implantation with Periosteum versus Matrix-Associated Autologous Chondrocyte Implantation: A Randomized Clinical Trial. Am. J. Sports Med. 48 (9), 2230–2241. 10.1177/0363546520928337 - DOI - PubMed
-
- Baumann C. A., Hinckel B. B., Bozynski C. C., Farr J. (2019). Articular Cartilage: Structure and Restoration. Germany: Springer.
LinkOut - more resources
Full Text Sources