

Clinical Profile and Prognosis of a Real-World Cohort of Patients With Moderate or Severe Cancer Therapy-Induced Cardiac Dysfunction
- PMID: 34778393
- PMCID: PMC8585751
- DOI: 10.3389/fcvm.2021.721080
Clinical Profile and Prognosis of a Real-World Cohort of Patients With Moderate or Severe Cancer Therapy-Induced Cardiac Dysfunction
Abstract
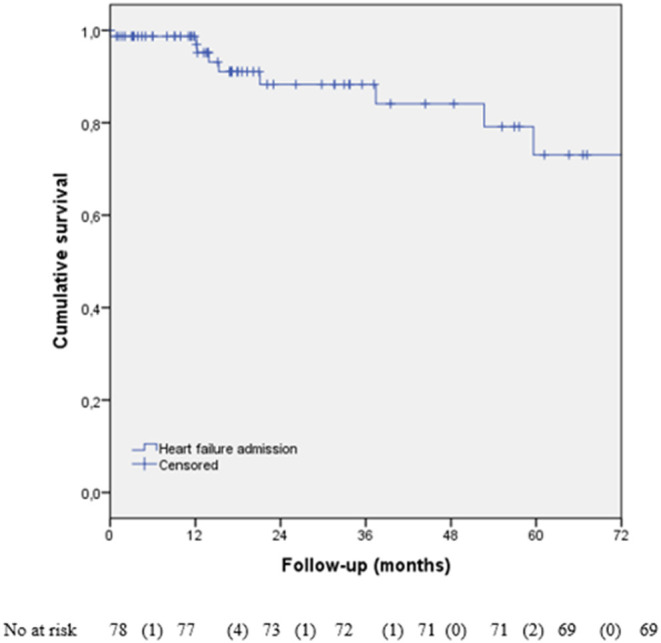
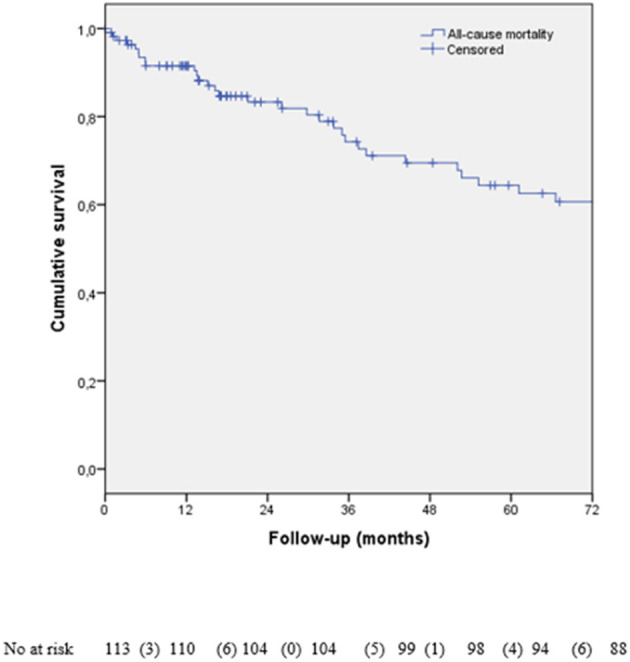
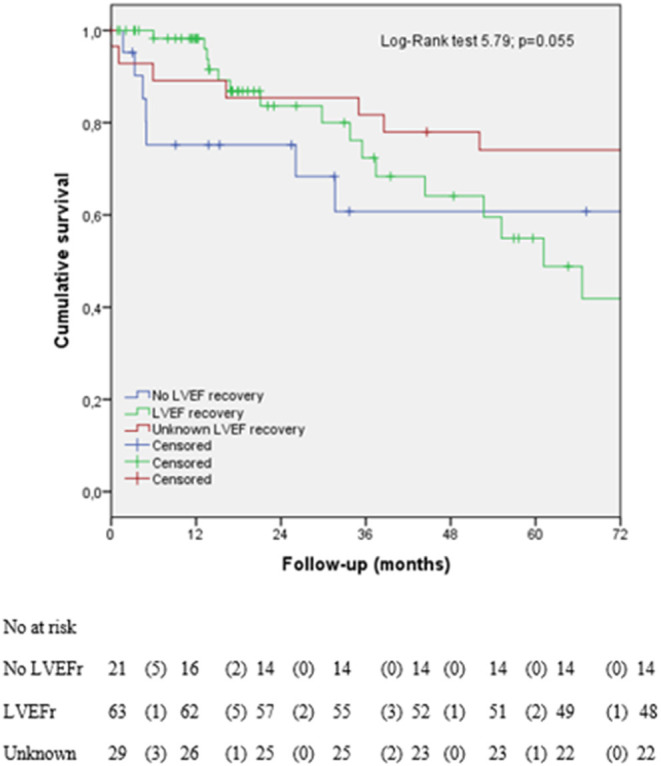
Introduction and Objectives: Cancer therapy-related cardiac dysfunction (CTRCD) is a common cause of cancer treatment withdrawal, related to the poor outcomes. The cardiac-specific treatment could recover the left ventricular ejection fraction (LVEF). We analyzed the clinical profile and prognosis of patients with CTRCD in a real-world scenario. Methods: A retrospective study that include all the cancer patients diagnosed with CTRCD, defined as LVEF < 50%. We analyzed the cardiac and oncologic treatments, the predictors of mortality and LVEF recovery, hospital admission, and the causes of mortality (cardiovascular (CV), non-CV, and cancer-related). Results: We included 113 patients (82.3% women, age 49.2 ± 12.1 years). Breast cancer (72.6%) and anthracyclines (72.6%) were the most frequent cancer and treatment. Meantime to CTRCD was 8 months, with mean LVEF of 39.4 ± 9.2%. At diagnosis, 27.4% of the patients were asymptomatic. Cardiac-specific treatment was started in 66.4% of patients, with LVEF recovery-rate of 54.8%. Higher LVEF at the time of CTRCD, shorter time from cancer treatment to diagnosis of CTRCD, and younger age were the predictors of LVEF recovery. The hospitalization rate was 20.4% (8.8% linked to heart failure). Treatment with trastuzumab and lower LVEF at diagnosis of CTRCD were the predictors of mortality. Thirty point nine percent of patients died during the 26 months follow-up. The non-CV causes and cancer-related were more frequent than CV ones. Conclusions: Cardiac-specific treatment achieves LVEF recovery in more than half of the patients. LVEF at the diagnosis of CTRCD, age, and time from the cancer treatment initiation to CTRCD were the predictors of LVEF recovery. The CV-related deaths were less frequent than the non-CV ones. Trastuzumab treatment and LVEF at the time of CTRCD were the predictors of mortality.
Keywords: cancer therapies; cancer therapy-related cardiac dysfunction; cardio-oncology; cardiotoxicity; left ventricular systolic dysfunction (LVSD).
Copyright © 2021 Esteban-Fernández, Carvajal Estupiñan, Gavira-Gómez, Pernas, Moliner, Garay, Sánchez-González, Fernández-Rozas and González-Costello.
Conflict of interest statement
SP has received a travel and accommodation grant from Novartis and advisor/consultant role for AstraZeneca, Daiichi-Sankyo, Polyphor, Roche, and Seattle Genetics. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, et al. . 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines. Eur Heart J. (2016) 37:2768–801. 10.1093/eurheartj/ehw211 - DOI - PubMed