

Disease- and Therapy-Specific Impact on Humoral Immune Responses to COVID-19 Vaccination in Hematologic Malignancies
- PMID: 34778797
- PMCID: PMC8580617
- DOI: 10.1158/2643-3230.BCD-21-0139
Disease- and Therapy-Specific Impact on Humoral Immune Responses to COVID-19 Vaccination in Hematologic Malignancies
Abstract
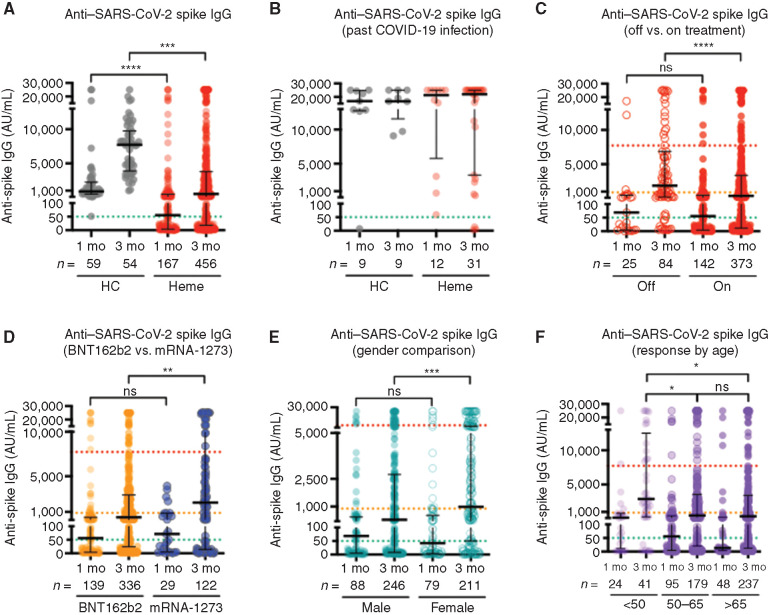
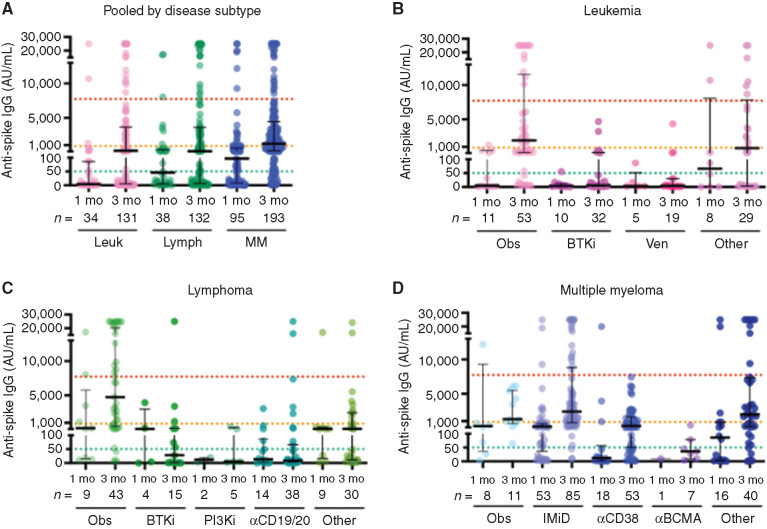
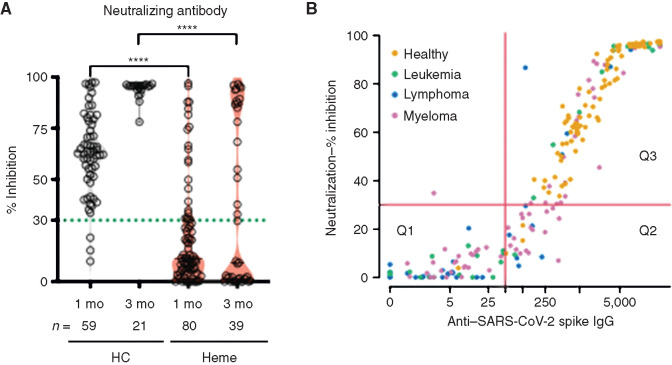
Coronavirus disease-19 (COVID-19) vaccine response data for patients with hematologic malignancy, who carry high risk for severe COVID-19 illness, are incomplete. In a study of 551 hematologic malignancy patients with leukemia, lymphoma, and multiple myeloma, anti-SARS-CoV-2 spike IgG titers and neutralizing activity were measured at 1 and 3 months from initial vaccination. Compared with healthy controls, patients with hematologic malignancy had attenuated antibody titers at 1 and 3 months. Furthermore, patients with hematologic malignancy had markedly diminished neutralizing capacity of 26.3% at 1 month and 43.6% at 3 months, despite positive seroconversion rates of 51.5% and 68.9% at the respective time points. Healthy controls had 93.2% and 100% neutralizing capacity at 1 and 3 months, respectively. Patients with leukemia, lymphoma, and multiple myeloma on observation had uniformly blunted responses. Treatment with Bruton tyrosine kinase inhibitors, venetoclax, phosphoinositide 3-kinase inhibitors, anti-CD19/CD20-directed therapies, and anti-CD38/B-cell maturation antigen-directed therapies substantially hindered responses, but single-agent immunomodulatory agents did not.
Significance: Patients with hematologic malignancy have compromised COVID-19 vaccine responses at baseline that are further suppressed by active therapy, with many patients having insufficient neutralizing capacity despite positive antibody titers. Refining vaccine response parameters is critical to guiding clinical care, including the indication for booster vaccines, for this vulnerable population.See related article by Tamari et al., p. 577. This article is highlighted in the In This Issue feature, p. 549.
©2021 American Association for Cancer Research.
Figures
Comment on
-
Predictors of Humoral Response to SARS-CoV-2 Vaccination after Hematopoietic Cell Transplantation and CAR T-cell Therapy.Blood Cancer Discov. 2021 Sep 13;2(6):577-585. doi: 10.1158/2643-3230.BCD-21-0142. eCollection 2021 Nov. Blood Cancer Discov. 2021. PMID: 34778798 Free PMC article.
References
-
- Rugge M, Zorzi M, Guzzinati S.SARS-CoV-2 infection in the Italian Veneto region: adverse outcomes in patients with cancer. Nat Cancer 2020;1:784–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
