

Insights from patients screened but not randomised in the HYPERION trial
- PMID: 34778914
- PMCID: PMC8590986
- DOI: 10.1186/s13613-021-00947-w
Insights from patients screened but not randomised in the HYPERION trial
Abstract
Background: Few data are available about outcomes of patients screened for, but not enrolled in, randomised clinical trials.
Methods: We retrospectively reviewed patients who had non-inclusion criteria for the HYPERION trial comparing 33 °C to 37 °C in patients comatose after cardiac arrest in non-shockable rhythm, due to any cause. A good neurological outcome was defined as a day-90 Cerebral Performance Category score of 1 or 2.
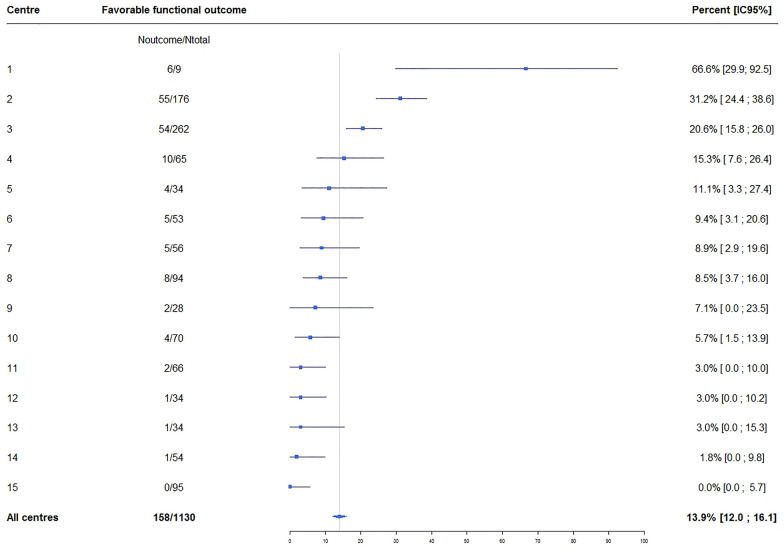
Results: Of the 1144 patients with non-inclusion criteria, 1130 had day-90 information and, among these, 158 (14%) had good functional outcomes, compared to 7.9% overall in the HYPERION trial (10.2% with and 5.7% without hypothermia). Considerable centre-to-centre variability was found in the proportion of non-included patients who received hypothermia (0% to 83.8%) and who had good day-90 functional outcomes (0% to 31.3%). The proportion of patients with a good day-90 functional outcome was significantly higher with than without hypothermia (18.5% vs. 11.9%, P = 0.003).
Conclusion: Our finding of better functional outcomes without than with inclusion in the HYPERION trial, despite most non-inclusion criteria being of adverse prognostic significance (e.g., long no-flow and low-flow times and haemodynamic instability), raises important questions about the choice of patient selection criteria and the applicability of trial results to everyday practice. At present, reserving hypothermia for patients without predictors of poor prognosis seems open to criticism.
Keywords: Cardiac arrest; Targeted temperature management; Therapeutic hypothermia.
© 2021. The Author(s).
Conflict of interest statement
All authors have completed and submitted the ICMJE Form for disclosure of potential conflicts of interest. Dr. Lascarrou reports lecture fees from BD and Zoll. Others authors declare no conflict of interest.
References
LinkOut - more resources
Full Text Sources
