

Novel genetic variants in MAPT and alterations in tau phosphorylation in amyotrophic lateral sclerosis post-mortem motor cortex and cerebrospinal fluid
- PMID: 34779076
- PMCID: PMC8877756
- DOI: 10.1111/bpa.13035
Novel genetic variants in MAPT and alterations in tau phosphorylation in amyotrophic lateral sclerosis post-mortem motor cortex and cerebrospinal fluid
Abstract
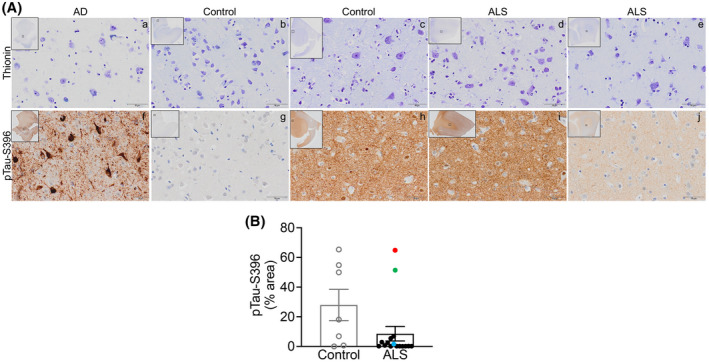
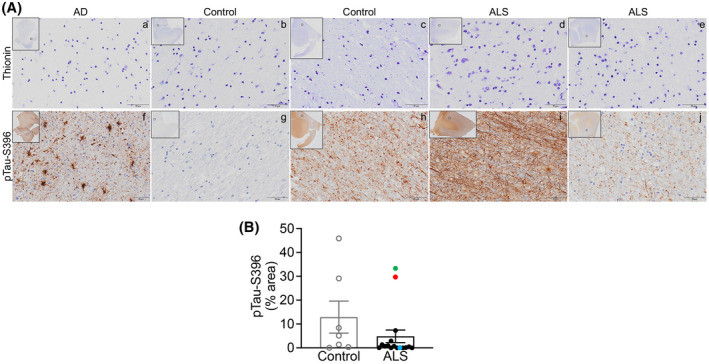
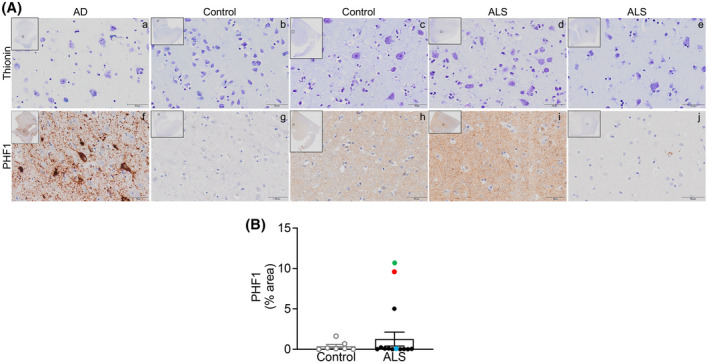
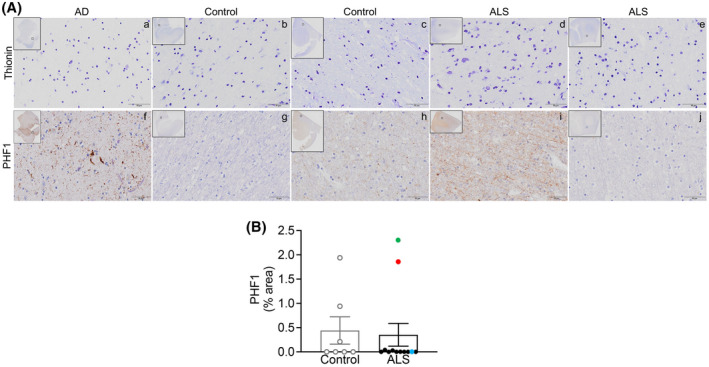
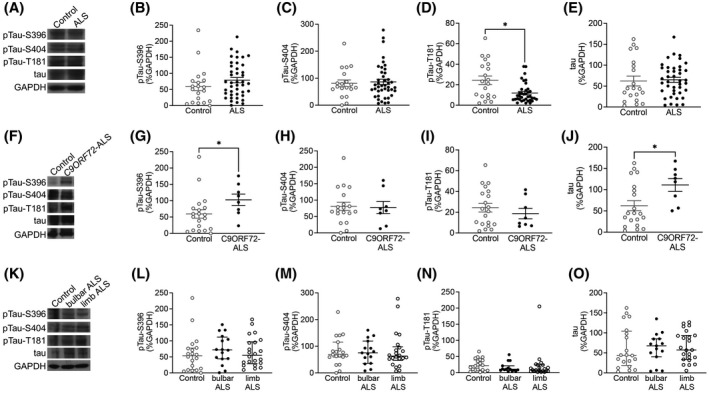
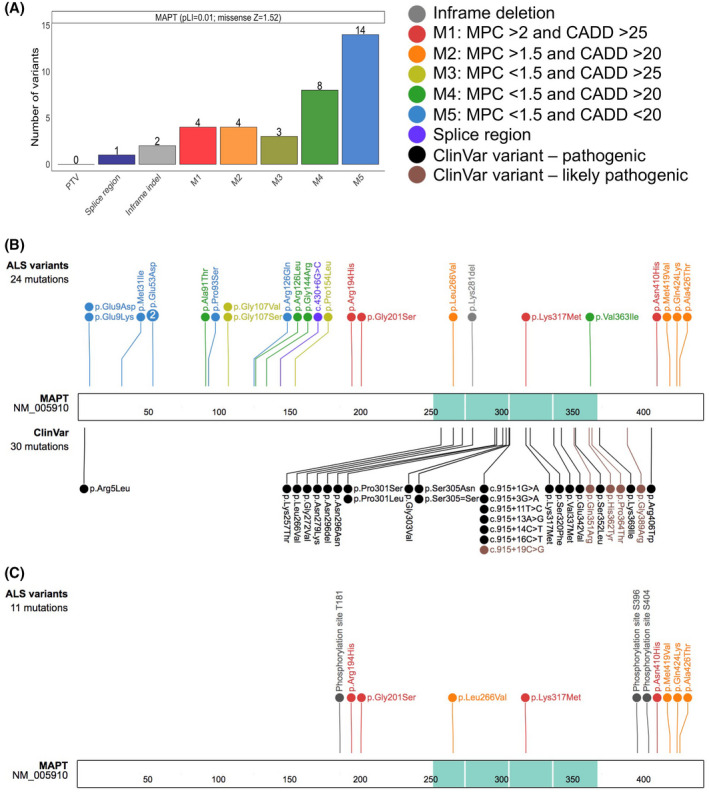
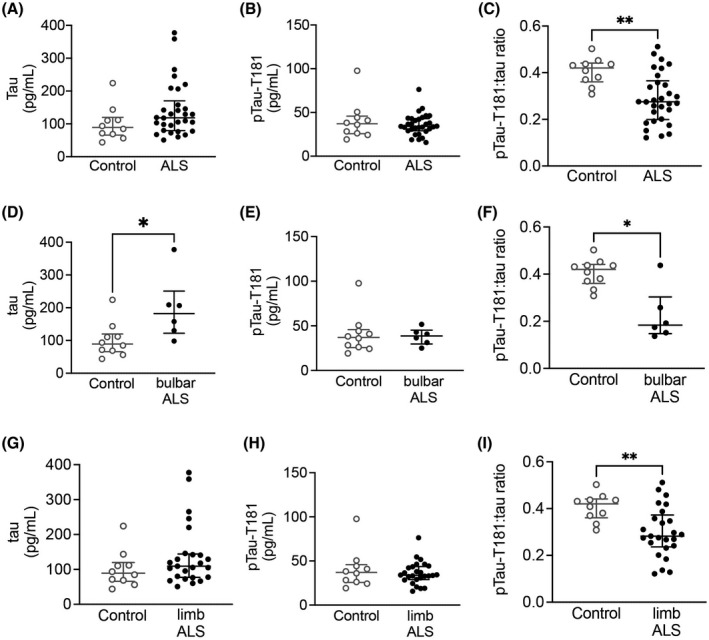
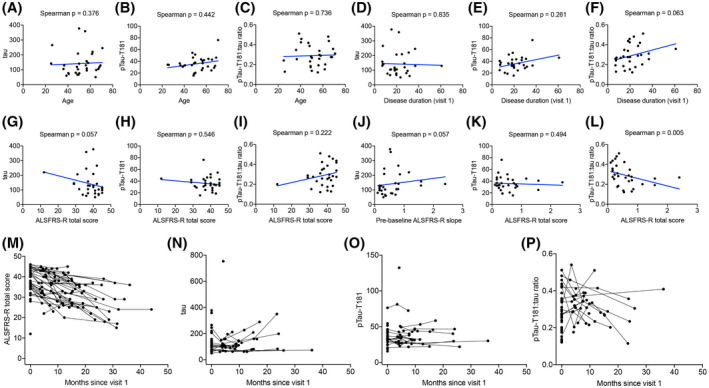
Although the molecular mechanisms underlying amyotrophic lateral sclerosis (ALS) are not yet fully understood, several studies report alterations in tau phosphorylation in both sporadic and familial ALS. Recently, we have demonstrated that phosphorylated tau at S396 (pTau-S396) is mislocalized to synapses in ALS motor cortex (mCTX) and contributes to mitochondrial dysfunction. Here, we demonstrate that while there was no overall increase in total tau, pTau-S396, and pTau-S404 in ALS post-mortem mCTX, total tau and pTau-S396 were increased in C9ORF72-ALS. Additionally, there was a significant decrease in pTau-T181 in ALS mCTX compared controls. Furthermore, we leveraged the ALS Knowledge Portal and Project MinE data sets and identified ALS-specific genetic variants across MAPT, the gene encoding tau. Lastly, assessment of cerebrospinal fluid (CSF) samples revealed a significant increase in total tau levels in bulbar-onset ALS together with a decrease in CSF pTau-T181:tau ratio in all ALS samples, as reported previously. While increases in CSF tau levels correlated with a faster disease progression as measured by the revised ALS functional rating scale (ALSFRS-R), decreases in CSF pTau-T181:tau ratio correlated with a slower disease progression, suggesting that CSF total tau and pTau-T181 ratio may serve as biomarkers of disease in ALS. Our findings highlight the potential role of pTau-T181 in ALS, as decreases in CSF pTau-T181:tau ratio may reflect the significant decrease in pTau-T181 in post-mortem mCTX. Taken together, these results indicate that tau phosphorylation is altered in ALS post-mortem mCTX as well as in CSF and, importantly, the newly described pathogenic or likely pathogenic variants identified in MAPT in this study are adjacent to T181 and S396 phosphorylation sites further highlighting the potential role of these tau functional domains in ALS.
Keywords: amyotrophic lateral sclerosis; biomarker; tau.
© 2021 The Authors. Brain Pathology published by John Wiley & Sons Ltd on behalf of International Society of Neuropathology.
Conflict of interest statement
T.G.I. serves as member of a Lilly Monitoring Committee (DMC). B.T.H. is a member of Novartis, Dewpoint, and Cell Signaling Scientific Advisory Board (SAB), and of Biogen DMC, and acts as consultant for US DoJ, Takeda, Virgil, W20, and Seer; he receives grants from Abbvie, F prime, NIH, Tau consortium, Cure Alzheimer's fund, Brightfocus, and JPB foundations. S.E.A. has received honoraria and/or travel expenses for lectures from Abbvie, Eisai, and Biogen and has served on SAB of Cortexyme and vTv, and as consultant for Athira, Cassava, Cognito Therapeutics, EIP Pharma and Orthogonal Neuroscience, and has received research grant support from NIH, Alzheimer's Association, Alzheimer's Drug Discovery Foundation, Abbvie, Amylyx, EIP Pharma, Merck, Janssen/Johnson & Johnson, Novartis, and vTv. T.S.J. is on the scientific advisory board of Cognition Therapeutics and receives collaborative grant funding from European Research Council, UK Dementia Research Institute, and Autifony. M.E.C. acts as consultant for Aclipse, Mt Pharma, Immunity Pharma Ltd., Orion, Anelixis, Cytokinetics, Biohaven, Wave, Takeda, Avexis, Revelasio, Pontifax, Biogen, Denali, Helixsmith, Sunovian, Disarm, ALS Pharma, RRD, Transposon, and Quralis, and as DSBM Chair for Lilly. J.D.B. has received personal fees from Biogen, Clene Nanomedicine, and MT Pharma Holdings of America, and grant support from Alexion, Biogen, MT Pharma of America, Anelixis Therapeutics, Brainstorm Cell Therapeutics, Genentech, nQ Medical, NINDS, Muscular Dystrophy Association, ALS One, Amylyx Therapeutics, ALS Association, and ALS Finding a Cure. G.S‐V. is a consultant for MarvelBiome. None of these had any influence over the current paper.
Figures
Similar articles
-
Targeting Tau Mitigates Mitochondrial Fragmentation and Oxidative Stress in Amyotrophic Lateral Sclerosis.Mol Neurobiol. 2022 Jan;59(1):683-702. doi: 10.1007/s12035-021-02557-w. Epub 2021 Nov 10. Mol Neurobiol. 2022. PMID: 34757590
-
Plasma tau and phosphorylated tau at T181 are altered in amyotrophic lateral sclerosis.medRxiv [Preprint]. 2025 Jun 27:2025.06.26.25330363. doi: 10.1101/2025.06.26.25330363. medRxiv. 2025. PMID: 40666341 Free PMC article. Preprint.
-
Significance of CSF NfL and tau in ALS.J Neurol. 2018 Nov;265(11):2633-2645. doi: 10.1007/s00415-018-9043-0. Epub 2018 Sep 5. J Neurol. 2018. PMID: 30187162
-
CSF markers in amyotrophic lateral sclerosis.J Neural Transm (Vienna). 2012 Jul;119(7):747-57. doi: 10.1007/s00702-012-0806-y. Epub 2012 May 4. J Neural Transm (Vienna). 2012. PMID: 22555610 Review.
-
Biochemical markers in CSF of ALS patients.Curr Med Chem. 2008;15(18):1788-801. doi: 10.2174/092986708785133031. Curr Med Chem. 2008. PMID: 18691039 Review.
Cited by
-
Shared genetic risk loci between Alzheimer's disease and related dementias, Parkinson's disease, and amyotrophic lateral sclerosis.Alzheimers Res Ther. 2023 Jun 16;15(1):113. doi: 10.1186/s13195-023-01244-3. Alzheimers Res Ther. 2023. PMID: 37328865 Free PMC article.
-
Cerebral Tau Deposition in Comorbid Progressive Supranuclear Palsy and Amyotrophic Lateral Sclerosis: An [18F]-Flortaucipir and 7T MRI Study.Neurodegener Dis. 2023;23(3-4):35-42. doi: 10.1159/000536614. Epub 2024 Mar 25. Neurodegener Dis. 2023. PMID: 38527450 Free PMC article.
-
CSF and blood levels of Neurofilaments, T-Tau, P-Tau, and Abeta-42 in amyotrophic lateral sclerosis: a systematic review and meta-analysis.J Transl Med. 2024 Oct 21;22(1):953. doi: 10.1186/s12967-024-05767-7. J Transl Med. 2024. PMID: 39434139 Free PMC article.
-
Modulation of histone H3K4 dimethylation by spermidine ameliorates motor neuron survival and neuropathology in a mouse model of ALS.J Biomed Sci. 2022 Dec 20;29(1):106. doi: 10.1186/s12929-022-00890-3. J Biomed Sci. 2022. PMID: 36536341 Free PMC article.
-
CSF p-tau as a potential cognition impairment biomarker in ALS.Front Neurol. 2022 Nov 1;13:991143. doi: 10.3389/fneur.2022.991143. eCollection 2022. Front Neurol. 2022. Retraction in: Front Neurol. 2024 Mar 04;15:1392563. doi: 10.3389/fneur.2024.1392563. PMID: 36388201 Free PMC article. Retracted.
References
-
- Brown RH Jr, Al‐Chalabi A. Amyotrophic lateral sclerosis. N Engl J Med. 2017;377:1602. - PubMed
-
- Nakamura S, Wate R, Kaneko S, Ito H, Oki M, Tsuge A, et al. An autopsy case of sporadic amyotrophic lateral sclerosis associated with the I113T SOD1 mutation. Neuropathology. 2014;34:58–63. - PubMed
-
- Bodakuntla S, Jijumon AS, Villablanca C, Gonzalez‐Billault C, Janke C, et al. Microtubule‐associated proteins: structuring the cytoskeleton. Trends Cell Biol. 2019;29:804–19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
