

Glycated haemoglobin levels among 3295 hospitalized COVID-19 patients, with and without diabetes, and risk of severe infection, admission to an intensive care unit and all-cause mortality
- PMID: 34779086
- PMCID: PMC8653248
- DOI: 10.1111/dom.14604
Glycated haemoglobin levels among 3295 hospitalized COVID-19 patients, with and without diabetes, and risk of severe infection, admission to an intensive care unit and all-cause mortality
Abstract
Aim: To determine the risk of adverse outcomes across the spectrum of glycated haemoglobin (HbA1c) levels among hospitalized COVID-19 patients with and without diabetes.
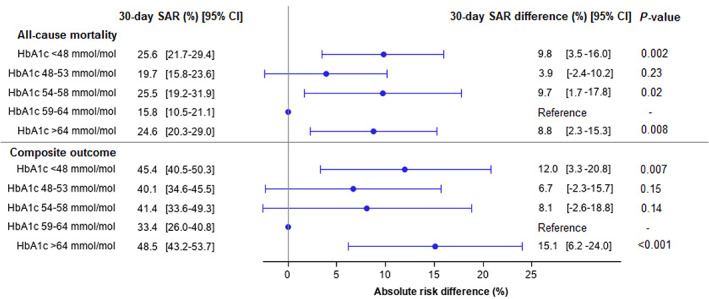
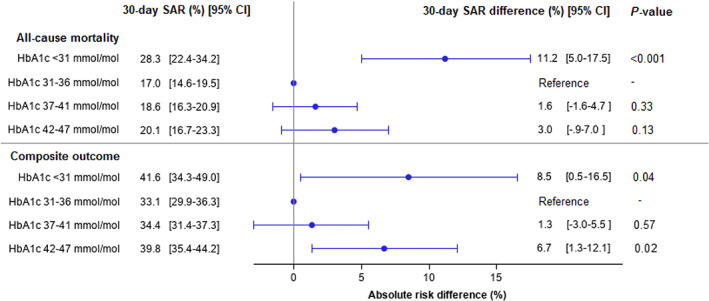
Materials and methods: Danish nationwide registries were used to study the association between HbA1c levels and 30-day risk of all-cause mortality and the composite of severe COVID-19 infection, intensive care unit (ICU) admission and all-cause mortality. The study population comprised patients hospitalized with COVID-19 (3 March 2020 to 31 December 2020) with a positive polymerase chain reaction (PCR) test and an available HbA1c ≤ 6 months before the first positive PCR test. All patients had at least 30 days of follow-up. Among patients with diabetes, HbA1c was categorized as <48 mmol/mol, 48 to 53 mmol/mol, 54 to 58 mmol/mol, 59 to 64 mmol/mol (reference) and >64 mmol/mol. Among patients without diabetes, HbA1c was stratified into <31 mmol/mol, 31 to 36 mmol/mol (reference), 37 to 41 mmol/mol and 42 to 47 mmol/mol. Thirty-day standardized absolute risks and standardized absolute risk differences are reported.
Results: We identified 3295 hospitalized COVID-19 patients with an available HbA1c (56.2% male, median age 73.9 years), of whom 35.8% had diabetes. The median HbA1c was 54 and 37 mmol/mol among patients with and without diabetes, respectively. Among patients with diabetes, the standardized absolute risk difference of the composite outcome was higher with HbA1c < 48 mmol/mol (12.0% [95% confidence interval {CI} 3.3% to 20.8%]) and HbA1c > 64 mmol/mol (15.1% [95% CI 6.2% to 24.0%]), compared with HbA1c 59 to 64 mmol/mol (reference). Among patients without diabetes, the standardized absolute risk difference of the composite outcome was greater with HbA1c < 31 mmol/mol (8.5% [95% CI 0.5% to 16.5%]) and HbA1c 42 to 47 mmol/mol (6.7% [95% CI 1.3% to 12.1%]), compared with HbA1c 31 to 36 mmol/mol (reference).
Conclusions: Patients with COVID-19 and HbA1c < 48 mmol/mol or HbA1c > 64 mmol/mol had a higher associated risk of the composite outcome. Similarly, among patients without diabetes, varying HbA1c levels were associated with higher risk of the composite outcome.
Keywords: antidiabetic drug; cardiovascular disease; database research; glycaemic control; hypoglycaemia; population study.
© 2021 John Wiley & Sons Ltd.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Effect of diabetes duration on the relationship between glycaemic control and risk of death in older adults with type 2 diabetes.Diabetes Obes Metab. 2020 Feb;22(2):231-242. doi: 10.1111/dom.13891. Epub 2019 Nov 18. Diabetes Obes Metab. 2020. PMID: 31596048
-
Associations between usual glycated haemoglobin and cardiovascular disease in patients with type 2 diabetes mellitus: A 10-year diabetes cohort study.Diabetes Obes Metab. 2020 Dec;22(12):2325-2334. doi: 10.1111/dom.14157. Epub 2020 Sep 17. Diabetes Obes Metab. 2020. PMID: 32744402
-
Glucagon-like-peptide-1 receptor agonists versus dipeptidyl peptidase-4 inhibitors and cardiovascular outcomes in diabetes in relation to achieved glycemic control. A Danish nationwide study.J Diabetes. 2024 Jun;16(6):e13560. doi: 10.1111/1753-0407.13560. J Diabetes. 2024. PMID: 38751369 Free PMC article.
-
Strategies for overcoming therapeutic inertia in type 2 diabetes: A systematic review and meta-analysis.Diabetes Obes Metab. 2021 Sep;23(9):2137-2154. doi: 10.1111/dom.14455. Epub 2021 Jun 27. Diabetes Obes Metab. 2021. PMID: 34180129
-
Elevated HbA1c levels in pre-Covid-19 infection increases the risk of mortality: A sistematic review and meta-analysis.Diabetes Metab Res Rev. 2022 Jan;38(1):e3476. doi: 10.1002/dmrr.3476. Epub 2021 May 28. Diabetes Metab Res Rev. 2022. PMID: 34018307 Free PMC article.
Cited by
-
Risk phenotypes of diabetes and association with COVID-19 severity and death: an update of a living systematic review and meta-analysis.Diabetologia. 2023 Aug;66(8):1395-1412. doi: 10.1007/s00125-023-05928-1. Epub 2023 May 19. Diabetologia. 2023. PMID: 37204441 Free PMC article.
-
The Role of Glycemic Control in Inflammation Markers and Clinical Outcomes in Type 2 Diabetes Patients with Severe COVID-19.Biomedicines. 2025 Apr 6;13(4):886. doi: 10.3390/biomedicines13040886. Biomedicines. 2025. PMID: 40299484 Free PMC article.
-
Association between antidiabetic drug use and the risk of COVID-19 hospitalization in the INSIGHT Clinical Research Network in New York City.Diabetes Obes Metab. 2022 Jul;24(7):1402-1405. doi: 10.1111/dom.14704. Epub 2022 Apr 25. Diabetes Obes Metab. 2022. PMID: 35373892 Free PMC article. No abstract available.
-
Random Blood Glucose, but Not HbA1c, Was Associated with Mortality in COVID-19 Patients with Type 2 Diabetes Mellitus-A Retrospective Study.Pathophysiology. 2023 Apr 6;30(2):136-143. doi: 10.3390/pathophysiology30020012. Pathophysiology. 2023. PMID: 37092526 Free PMC article.
-
The clinical features and outcomes of diabetes patients infected with COVID-19: a systematic review and meta-analysis comprising 192,693 patients.Front Med (Lausanne). 2025 Jan 29;12:1523139. doi: 10.3389/fmed.2025.1523139. eCollection 2025. Front Med (Lausanne). 2025. PMID: 39944495 Free PMC article.
References
-
- World Health Organization 2020. https://www.who.int/director-general/speeches/detail/who-director-genera.... Accessed November 2, 2021
-
- Currie CJ, Peters JR, Tynan A, et al. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet. 2010;375(9713):481‐489. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
