

Sex Differences in Cumulative Exposure to Metabolic Risk Factors Before Hypertension Onset: The Cohort of the Tehran Lipid and Glucose Study
- PMID: 34779244
- PMCID: PMC9075390
- DOI: 10.1161/JAHA.121.021922
Sex Differences in Cumulative Exposure to Metabolic Risk Factors Before Hypertension Onset: The Cohort of the Tehran Lipid and Glucose Study
Abstract
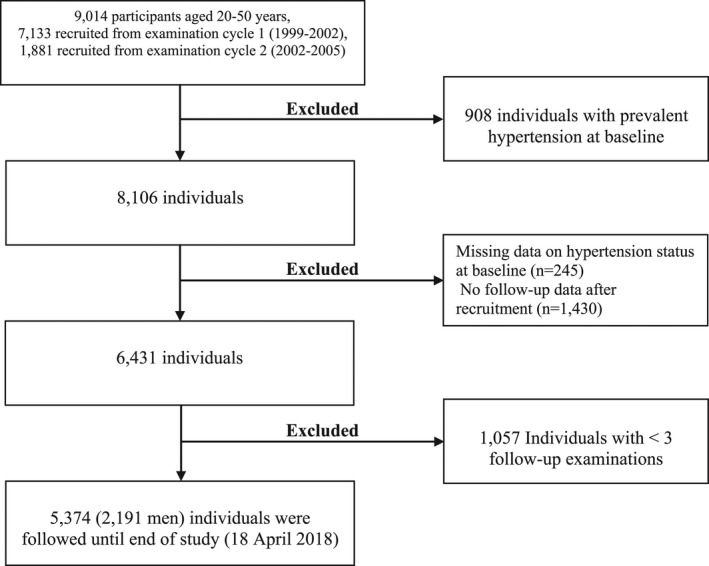
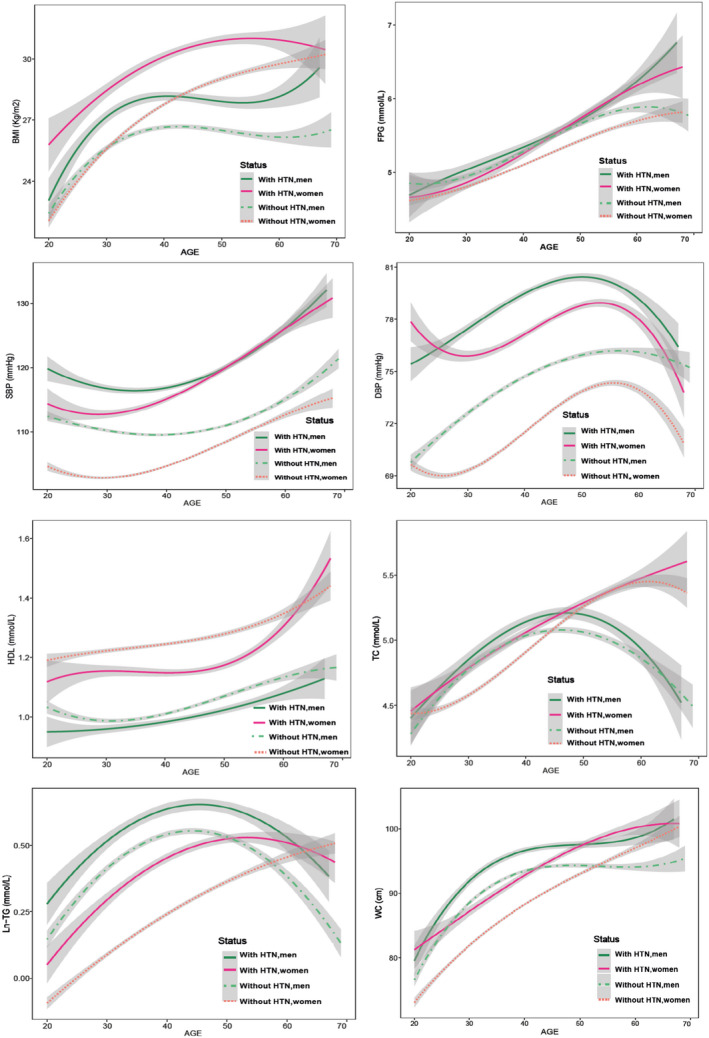
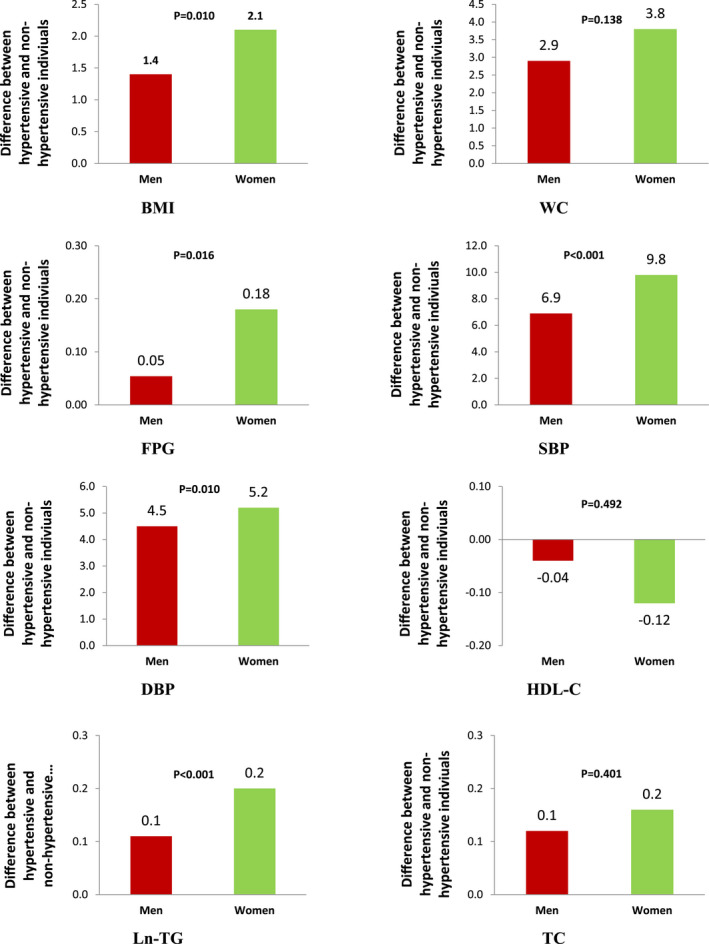
Background Previous studies have shown a sex difference in the association between hypertension and cardiovascular disease; however, the precise mechanism remains unclear. Because there are strong associations between metabolic risk factors (MRFs) and hypertension, a sex-specific analysis of MRFs before hypertension onset could offer new insights and expand our understanding of sex differences in cardiovascular disease. We evaluated cumulative exposure to major MRFs and rate of change of those factors, including body mass index, waist circumference, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, total cholesterol, triglycerides, and high-density lipoprotein cholesterol among individuals who did and did not develop hypertension at follow-up. Methods and Results We included 5374 participants (2191 men) initially without hypertension with age range of 20-50 years at baseline who participated in the Tehran Lipid and Glucose Study, and had been examined at least 3 times during the study period (1999-2018). In both sexes, the cumulative exposure to all MRFs (except for fasting plasma glucose and high-density lipoprotein cholesterol in men) were higher in those who developed hypertension, compared with those who did not develop hypertension. However, women experienced greater cumulative exposure to major MRFs, compared with their male counterparts. Also, they experienced a faster increase in waist circumference, systolic blood pressure, diastolic blood pressure, and high-density lipoprotein cholesterol than men. Furthermore, rapid increase in systolic blood pressure began earlier in women than men, at the age of 30 years. We also found that those men who developed hypertension experienced unfavorable change in major MRFs during young adulthood (<50 years of age). Conclusions Women exhibited more metabolic disturbances than men before onset of hypertension, which may explain the stronger impact of hypertension for major types of cardiovascular disease in women, compared with men.
Keywords: burden; hypertension; metabolic; risk factor; trajectory.
Figures
References
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, et al. Heart disease and stroke statistics‐2018 update: a report from the American Heart Association. Circulation. 2018;137:e67–e492. - PubMed
-
- Bennett JE, Stevens GA, Mathers CD, Bonita R, Rehm J, Kruk ME, Riley LM, Dain K, Kengne AP, Chalkidou K, et al. NCD countdown 2030: worldwide trends in non‐communicable disease mortality and progress towards sustainable development goal target 3.4. Lancet. 2018;392:1072–1088. doi: 10.1016/S0140-6736(18)31992-5 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
