

Prognostic Role of Myocardial Edema as Evidenced by Early Cardiac Magnetic Resonance in Survivors of Out-of-Hospital Cardiac Arrest: A Multicenter Study
- PMID: 34779249
- PMCID: PMC8751964
- DOI: 10.1161/JAHA.121.021861
Prognostic Role of Myocardial Edema as Evidenced by Early Cardiac Magnetic Resonance in Survivors of Out-of-Hospital Cardiac Arrest: A Multicenter Study
Abstract
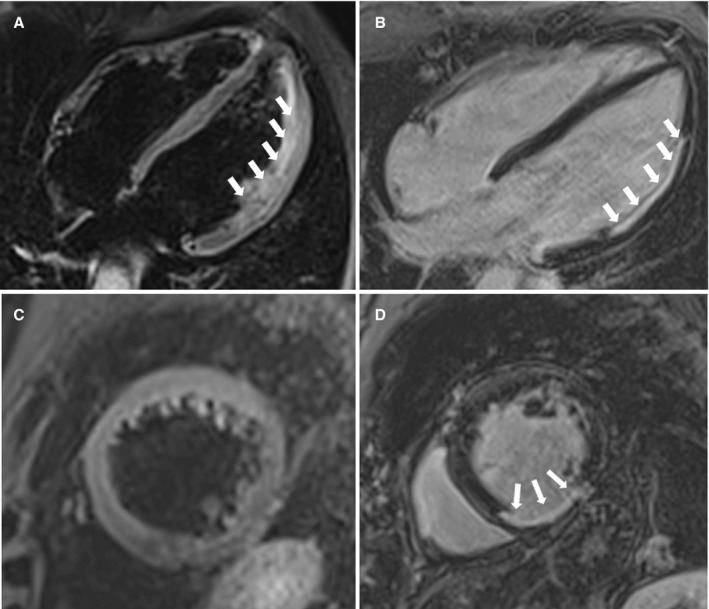
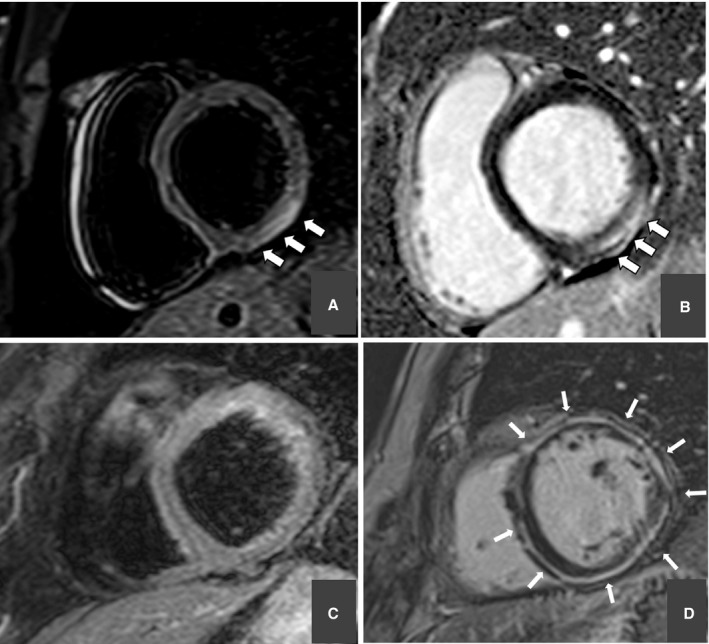
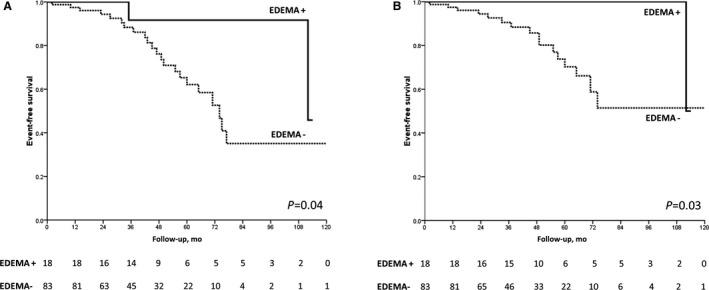
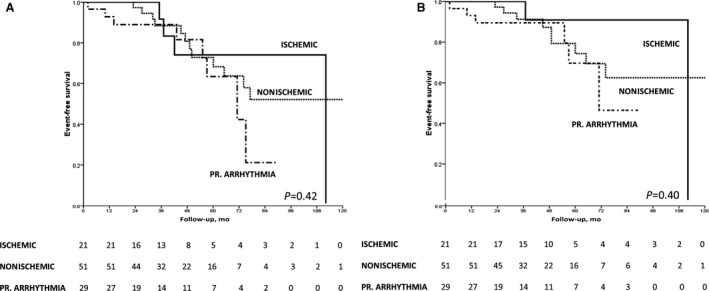
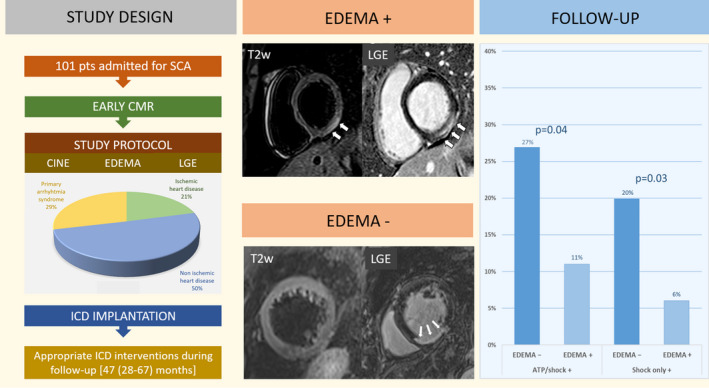
Background Sudden cardiac arrest (SCA) may be caused by an acute and reversible myocardial injury, a chronic and irreversible myocardial damage, or a primary ventricular arrhythmia. Cardiac magnetic resonance imaging may identify myocardial edema (ME), which denotes acute and reversible myocardial damage. We evaluated the arrhythmic outcome of SCA survivors during follow-up and tested the prognostic role of ME. Methods and Results We included a consecutive series of 101 (71% men, median age 47 years) SCA survivors from 9 collaborative centers who underwent early (<1 month) cardiac magnetic resonance imaging and received an implantable cardioverter-defibrillator (ICD). On T2-weighted sequences, ME was found in 18 of 101 (18%) patients. According to cardiac magnetic resonance imaging findings, the arrhythmic SCA was ascribed to acute myocardial injury (either ischemic [n=10] or inflammatory [n=8]), to chronic structural heart diseases (ischemic heart disease [n=11], cardiomyopathy [n=20], or other [n=23]), or to primarily arrhythmic syndrome (n=29). During a follow-up of 47 months (28 to 67 months), 24 of 101 (24%) patients received an appropriate ICD intervention. ME was associated with a significantly higher survival free from both any ICD interventions (log-rank=0.04) and ICD shocks (log-rank=0.03) and remained an independent predictor of better arrhythmic outcome after adjustment for left ventricular ejection fraction and late gadolinium enhancement. The risk of appropriate ICD intervention was unrelated to the type of underlying heart disease. Conclusions ME on early cardiac magnetic resonance imaging, which denotes an acute and transient arrhythmogenic substrate, predicted a favorable long-term arrhythmic outcome of SCA survivors. These findings may have a substantial impact on future guidelines on the management of SCA survivors.
Keywords: cardiac magnetic resonance; implantable cardioverter‐defibrillator; out‐of‐hospital cardiac arrest; prognosis; ventricular arrhythmia.
Figures
Comment in
-
The Bright Side of Myocardial Edema.J Am Heart Assoc. 2021 Nov 16;10(22):e023731. doi: 10.1161/JAHA.121.023731. Epub 2021 Nov 15. J Am Heart Assoc. 2021. PMID: 34779232 Free PMC article. No abstract available.
References
-
- Al‐Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB, Deal BJ, Dickfeld T, Field ME, Fonarow GC, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018;138:e211–e269. doi: 10.1161/CIR.0000000000000548 - DOI - PubMed
-
- Priori SG, Blomström‐Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2015;36:2793–2867. doi: 10.1093/eurheartj/ehv316 - DOI - PubMed
-
- Nolan JP, Neumar RW, Adrie C, Aibiki M, Berg RA, Böttiger BW, Callaway C, Clark RS, Geocadin RG, Jauch EC, et al. Post‐cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A scientific statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation. 2008;79:350–379. doi: 10.1016/j.resuscitation.2008.09.017 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
